Dr. Eka Musridharta, SpS Data Pribadi Tempat/Tgl Lahir : Jakarta, 1 Mei 1975 Alamat : Bulu Perindu Raya Blok N-3 Pondok Bambu, 13430 +68551075488 [email protected] Pendidikan Pendidikan Dokter Umum FKUI, Lulus 2009 Pendidikan Dokter Spesialis Neurologi FKUI, lulus 2006 Pendidikan Konsultan Intensive Care FKUI, Lulus 2009 Jabatan Staff Medik Departemen Neurologi RSCM Konsultan Neurofisiologi RS. Pusat Pertamina Konsultan Neurofisiologi RS. Menteng Mitra Afia

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dr. Eka Musridharta, SpSData Pribadi
Tempat/Tgl Lahir : Jakarta, 1 Mei 1975
Alamat : Bulu Perindu Raya Blok N-3
Pondok Bambu, 13430
+68551075488
Pendidikan
Pendidikan Dokter Umum FKUI, Lulus 2009
Pendidikan Dokter Spesialis Neurologi FKUI, lulus 2006
Pendidikan Konsultan Intensive Care FKUI, Lulus 2009
Jabatan
Staff Medik Departemen Neurologi RSCM
Konsultan Neurofisiologi RS. Pusat Pertamina
Konsultan Neurofisiologi RS. Menteng Mitra Afia

SIRS and Brain Injury
Dr Eka Musridharta, SpS KIC

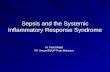
Sepsis: Defining a Disease Continuum
A clinical response arising from a nonspecific insult, including 2 of the following:
• Temperature 38oC or 36oC
• HR 90 beats/min
• Respirations 20/min
• WBC count 12,000/mm3 or4,000/mm3 or >10% immature neutrophils
SIRS = Systemic Inflammatory Response Syndrome
SIRS plus/with a presumed or confirmed infectious process
SepsisSIRSInfection/
Trauma/shock Severe Sepsis
Adapted from: Bone RC, et al. Chest 1992;101:1644Opal SM, et al. Crit Care Med 2000;28:S81

Sepsis: Defining a Disease Continuum
Bone et al. Chest 1992;101:1644; Wheeler and Bernard. N Engl J Med 1999;340:207
SepsisSIRSInfection/
Trauma/shock Severe Sepsis
Sepsis with 1 sign of organ failureCardiovascular (refractory hypotension)
Renal
Respiratory
Hepatic
Hematologic
CNS
Metabolic acidosis
Septic Shock

ACCP/SCCM Consensus
Definitions
O InfectionO Inflammatory response to
microorganisms, or
O Invasion of normally sterile tissues
O Systemic Inflammatory
Response Syndrome (SIRS)O Systemic response to a variety of
processes
O SepsisO Infection plus
O 2 SIRS criteria
O Severe SepsisO SepsisO Organ dysfunction
O Septic shockO SepsisO Hypotension despite fluid
resuscitation
O Multiple Organ Dysfunction Syndrome (MODS)O Altered organ function in an
acutely ill patientO Homeostasis cannot be
maintained without intervention
Bone RC et al. Chest. 1992;101:1644-55.

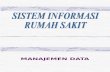
Clinical presentation
Sepsis / SIRS
SEPTIC SHOCK/MOF
Biologic sequelae
Monocyte activation
Monocyte deactivation
TNF-IL-1ßIL-6IL-8PAFiNOSCOX2
IL-1 raIL-10sTNFr-1/11TGF-IL-4
PROINFLAMMATORY
PROINFLAMMATORY
ANTI-INFLAMMATORY
ANTI-INFLAMMATORY CELL HYPORESPONSIVENESS / IMMUNOPARALYSIS
TNF-IL-1ßIL-6IL-8PAFiNOSCOX2
IL-1 raIL-10sTNFr-1/11TGF-IL-4
Imbalance between Pro-Inflamatory and Anti-inflamatory response
SIRS =SYSTEMIC INFLAMATORY
RESPONSE SYNDROME
CARS =COMPENSATED
ANTI-INFLAMATORYRESPONSE SYNDROME

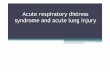
Mortality
Septic
Shock53-63%
20-53%Severe Sepsis
300,000
7-17%
Sepsis
400,000
Incidence
Balk, R.A. Crit Care Clin 2000;337:52
Mortality Increases in Septic Shock Patients

2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definition Conference. CCM 2003;31:1250-1256

CEREBRAL ENERGY METABOLISM
The brain comprises only 2% of body weight, but
receives 15% of cardiac output and uses 20%
of total body oxygen and 25% of total body
glucose.
Within normal levels of global CBF the brain
extracts about 50% of the oxygen and 10% of
the glucose from arterial blood.

Elevation of body temperature
occurring as a result of
hypothalamic coordination of
autonomic, neuroendocrine, and
behavioral responses in reaction to
physiological injury or invasion is
generally known as fever

Traditional thought is that the
“febrile response” is beneficial in
preventing the proliferation of
invading microorganisms, but
some caregivers consider fever
to be harmful

Fever and Brain Injury
“ Moreover, increasing evidence
suggest that fever (irrespective of
its cause) can directly and
adversely affect neurological
outcome in various types of
neurological injury”
Polderman, Lancet,2009

Pathophysiology of Fever
O Rise in temperature due to regulated increase in patient’s hypothalamic set point
O oxygen consumption
O metabolic rate
O heart rate
O cardiac output
O leukocyte count
O levell of C-Reactive Protein
O May be detrimental to a critically ill patient

Brain Temperature
Local brain temperature may exceed
core temperature by up to 2°C
This variance may increase in the injured brain
due to hyper-metabolism in injured areas
Polderman, Lancet,2009

Prevalence of Hyperthermia
O Defined as temperature increase of > 38.3°C or one full degree above baseline
O Occurs in up to 70% of all neurologically-injuries patients
O Typically not an isolated event but a sustained response for as long as 2 weeks
O Risk of hyperthermia may increase by 32% for each additional day in ICU
O Evidence suggests that fever worsens injury after ischemia or trauma
Mc Ilvoy,AACN Clin.Issues,2006Badjatia, Current Neur and Neurosurg Reports, 2009

Neurogenic Fever
O Non infectious source of fever
O Results from disruption in the hypothalamic
set point
O Injury to hypothalamus; unclear mechanism
O Patient response
O Increased temperature (may plateau),
resistant to antipyretics
O Absence of perspiration.

Elevated temperature exacerbates neuronal
injury caused by cerebral ischemia or
traumatic brain injury (TBI) and, conversely,
hypothermia acts as a neuroprotectant in such
cases.
Well-controlled animal models of global and
focal ischemia demonstrate a significantly
detrimental effect of hyperthermia on clinical
outcome and neuropathological changes

hyperthermia worsens outcome in cerebral ischemia:
increased neurotransmitter release
increased free radical production
opening of the blood-brain barrier
increased depolarizations within the
penumbra
impaired brain metabolism and second
messenger inhibition
cytoskeletal degradation

“the action of otherwise
neuroprotective drugs in ischemia may
be nullified by mild hyperthermia.”
brain temperature monitoring and treatment
of elevated temperature in patients suffering
from neurological insult may, therefore, help
prevent secondary injury.

Ischemic Stroke and Fever
O Fever on admission has been correlated with larger infarct sizes and increased mortality.
O Each 1°C increase in temperature “doubles the relative risk for poor functional outcome”
O Neuronal loss may be increased even when occurring 24 hours after original insult
O Maintaining normothermia after ischemia stabilizes the blood-brain barrier and reduces cerebral metabolism
Badjatia, CCM, 2009

Temperature elevations aggravate ischemic neuronal injury and exacerbate brain edema

TBI and Hyperthermia
O Intracranial blood volume increases with rise in temperature
O Causes a reduced compliance and increases ICP
O Elevates risk for further neuronal injury
O 13% increase in metabolic rate associated with every 1°C increase in body temperature
O Increases risk of secondary injury
O Rates as high as 68% have been reported within 72 hours of TBI
Thompson et all. J. Neurol Neurosurg Psychiatry, 2003.

TBI and Hyperthermia
O Fever occurring within first week of injury
has been associated with:
O Increased ICP
O Neurologic impairment
O Prolonged ICU stay
O Long-term poor outcome
O Recommendation is to treat fever
aggressively in this patient population
Badjatia, CCM, 2009

SAH and Hyperthermia
O Occurs in up to 70% of all patients in first 10
days
O Hyperthermia has been linked to increased
ICP after SAH
O Fever occurring late (4 to 6 days after injury)
in SAH patients has been associated with
cerebral vasospasm
Badjatia, CCM, 2009



Treating Fevers
O Pharmacological: O Linked to intact thermoregulatory
mechanismsO Such as Acetaminophen, Ibuprofen.
O Surface Cooling O Water blankets O Hydrogel pads
O IntravascularO Endovascular cathetersO Iced saline

Controled Normothermia
O “Traditional Therapy” has consisted of water
blankets and antipyretic, which have been
proven to have <40% success rates
O Advanced technology
O 75% reduction in fever.

Induced Hypothermia

Advanced Technology

Acetaminophen

32
Arachidonic Acid Cascades
PLA-2
COX-1
Constitutive
COX-2
Inducible
Lipoxyge-
nase
COX-3
Leukotriene Prostaglandin ProstaglandinProstacyclin
GI Mucosal
Protection
GI Mucosal
Immun
System
Inflamm
Plat aggreg and
Hemostasis
Vasodil &
endothelial
function
Platelet
Thromboxane
TXA-2 Mediate pain,
inflammation,
fever & regulate
cell growth
Brain
Mediate pain
and Fever
Acetamino
phen
Botting et al 2005: Benarroch, 2006
Vascular


Acetaminophen
O Acetaminophen is generally considered to be a weak inhibitor of the synthesis of prostaglandins (PGs).
O Acetaminophen also decreases PG concentrations in vivo, but, unlike the selective COX-2 inhibitors, acetaminophen does not suppress the inflammation of rheumatoid arthritis.
O Acetaminophen is a weak inhibitor of PG synthesis of COX-1 and COX-2 in broken cell systems, but, by contrast, therapeutic concentrations of acetaminophen inhibit PG synthesis in intact cells in vitro when the levels of the substrate arachidonic acid are low (less than about 5 μmol/L).
Graham, Garry G.; Scott, Kieran F. Am J of Therapeutics: 2005.12 - Issue 1: 46-55

Acetaminophen
O COX-3, a splice variant of COX-1, has been
suggested to be the site of action of
paracetamol.
O There is considerable evidence that the
analgesic effect of paracetamol is central
and is due to activation of descending
serotonergic pathways, but its primary site of
action may still be inhibition of PG synthesis.
Graham, Garry G.; Scott, Kieran F. Am J of Therapeutics: 2005.12 - Issue 1: 46-55

Acetaminophen and Clinical Settings

37
Acetaminophen Penetrates Readily Into the CSF of Children After I.V
Administration
O The children, aged 3 months to 12 years, who were undergoing surgery in the lower body using spinal anesthesia were given a single IV inject of paracet (15 mg/kg).
O CSF and venous blood samples were obtained between 5 min and 5 hours after injection.
O Paracetamol concentrations were determined by using a fluorescence polarization immunoassay.
Elina Kumpulainen, BMa,b, et al. Published online April 2, 2007PEDIATRICS Vol. 119 No. 4 April 2007, pp. 766-771 (doi:10.1542/peds.2006-3378)

Results
O Acetaminophen was detected in CSF from the earliest sample at 5 minutes, although in this sample acetaminophen concent was below the limit of quantification of 1.0 mg/L.
O Subsequent CSF acetaminophen concentr ranged between 1.3 and 18 mg/L (median: 7.2 mg/L), plasma concentr ranged between 2.4 and 33 mg/L, and CSF/plasma ratios ranged between 0.06 and 2.0.
O The highest CSF acetaminophen concentr was detected at 57 minutes.

Study Conclusions
O Acetaminophen permeates readily into the
CSF of children.
O This fast and extensive transfer enables the
rapid central analgesic and antipyretic
action of IV acetaminophen.







Summary• Hyperthermia may caused of increased O2 Consumption and
metabolism rate and may be detrimental to a critically ill
patient
• Occurs in up to 70% of all neurologically-injuries patients
• Hyperthermia poor outcome in brain injury.
• The modalities of treatment of hyperthermia are
pharmacological therapy, surface cooling and intravascular
cooling.
• Acetaminophen intravenous is the choice of drug if the
patient is unable to take oral or rectal and NSAIDs are
contraindicated.

Thank You

Related Documents