ELEKTROKARDIOGRAFI ELEKTROKARDIOGRAFI KELAKAR MEDAN Departemen Kardiologi dan Kedokteran Vaskuler Fakultas Kedokteran Universitas Sumatera Utara

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ELEKTROKARDIOGRAFIELEKTROKARDIOGRAFI
KELAKAR MEDANDepartemen Kardiologi dan Kedokteran Vaskuler
Fakultas KedokteranUniversitas Sumatera Utara

SA nodeSumber impuls normal/ alamiah , 60 – 100 / menit
AV nodeBisa mengeluarkan impuls 40-50x/menit
Berkas HisSerabut Purkinje
VentrikelBisa mengeluarkan impuls30 x/menit
Conduction System

P
Q S
R
TU P
DEFINISI KONFIGURASI EKG
Gel. P = defleksi akibat depolarisasi atrium Gel. Q(q) = defleksi negatif awal akibat depolarisasi ventrikel yg mendahului gel. (R)
Gel. R(r) = defleksi positif awal akibat depolarisasi ventrikelGel. S(s) = defleksi negatif awal akibat depolarisasi ventrikel yg mengikuti gel. (R)
Gel. R’(r’) = defleksi negatif awal akibat depolarisasi ventrikel yg mengi- kuti gel. (R) Gel.T = defleksi akibat repolarisasi ventr. Gel. U = defleksi (biasanya positif) sete- lah gel T dan mendahului gel P
-------- = depolarisasi atrium -------- = depolarisasi dan repolarisasi
ventrikel
-------- = depolarisasi ventrikel

NILAI NORMAL :
Gelombang P : durasi : 0.08 – 0.10 / 0,12 detik
tinggi (voltase) : < 2,5 mm
Interval PR : 0,12 – 0,20 detik
Kompleks QRS : durasi : 0,06 – 0,10 detik
tinggi : > 5 mm standard limb lead ; > 10 mm chest lead
Interval QT : ♀ < 0,42 ; ♂ < 0,44 detik
Interval QTc : QT √ RR
Gelombang T : 1/8 – 2/3 dari tinggi gelombang R
Segmen ST : isoelektris

Sandapan EKG (standar - 12 lead)
Sandapan bipolarSandapan bipolar
Merekam perbedaan potensial dari 2 elektrodaI = lengan kanan (-) lengan kiri (+)II = lengan kanan (-) tungkai kiri (+)III = lengan kiri (-) tungkai kiri (+)
Sandapan unipolarSandapan unipolar- Merekam potensial listrik pada satu elektroda
yang lain sebagai elektroda indiferen (0)- Ada dua sandapan: ekstremitas & prekordial
Sandapan unipolar ekstremitasavR, avL, avF
- Sandapan prekordialV1,V2,V3,V4,V5,V6




ECG interpretation…?
1. Calibration2. Rate and rhythm3. QRS axis4. P morphology5. PR interval6. QRS duration7. QRS morphology8. ST segment morphology9. T morphology10.Others: LVH, LV strain, BBB11.Conclusion: normal/abnormal

DEFINISI KONFIGURASI GELOMBANG EKG
Kertas EKGHorizontal menyatakan kecepatan kertas dalam waktu1 mm = 0,04 detik 5 mm = 0,2 detik
Vertikal menyatakan voltage elektris jantung dalam millivolt
10 mm = 1 mV
Pada pemeriksaan rutin kecepatan rekaman kertas EKG 25 mm/detik
1 mm = 0,1 mV
10 mm = 1 mV
1 mm = 0,04 detik
5 mm = 0,2 detik

Sebutkan iramanya : Sinus Rhythm
Irama Jantung

MENGHITUNG DENYUT JANTUNG DARI EKG :
a. Irama Sinus : 1.1500 / jarak RR (kotak kecil)
2. 300 / jarak RR (kotak besar)
b. Sinus aritmia : 1. Hitung jumlah RR dalam 5 detik atau,
2. Hitung jumlah RR dalam 6 detik atau,
3. Hitung jumlah RR dalam 10 detik,
kemudian
1. HR = (jumlah RR dalam 5 detik x 12), atau
2. HR = (jumlah RR dalam 6 detik x 10 atau), atau
3. HR = (jumlah RR dalam 10 detik x 6)

1 kotak besar = 300
2 kotak besar = 150
3 kotak besar = 100
4 kotak besar = 75
5 kotak besar = 60
6 kotak besar = 50
7 kotak besar = 43
8 kotak besar = 37
1 2 3 4 5 6 70 8
“Count off" method

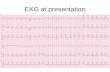
Normal Sinus RhythmLooking at the ECG you'll see that:•Rhythm - Regular •Rate - (60-100 bpm) •QRS Duration - Normal •P Wave - Visible before each QRS complex •P-R Interval - Normal (<5 small Squares. Anything above and this would be 1st degree block) •Indicates that the electrical signal is generated by the sinus node and travelling in a normal fashion in the heart.
Source: Male, 48 years old, Heart Rate: 65bpm, PR: 188ms, QRS: 92ms
1. SINUS RHYTHM

•Sinus TachycardiaAn excessive heart rate above 100 beats per minute (BPM) which originates from the SA node. Causes include stress, fright, illness and exercise. Not usually a surprise if it is triggered in response to regulatory changes e.g. shock. But if their is no apparent trigger then medications may be required to suppress the rhythm Looking at the ECG you'll see that:•Rhythm - Regular •Rate - More than 100 beats per minute •QRS Duration - Normal •P Wave - Visible before each QRS complex •P-R Interval - Normal •The impulse generating the heart beats are normal, but they are occurring at a faster pace than normal. Seen during exercise

•Sinus BradycardiaLooking at the ECG you'll see that:•Rhythm - Regular •Rate - less than 60 beats per minute •QRS Duration - Normal •P Wave - Visible before each QRS complex •P-R Interval - Normal •Usually benign and often caused by patients on beta blockers & healthy athletic person

AXIS JANTUNG
Stimulus depolarisasi dan repolarisasi didalam jantung menyebar ke berbagai arah didalam jantung sesuai dengan posisi anatomi jantung
Aksis jantung : 1. Aksis QRS
2. Aksis gelombang P
3. Aksis gelombang T
1. Aksis QRS : arah depolarisasi gelombang QRS pada frontal plane yang ditentukan oleh posisi anatomi jantung
2. Aksis P : arah depolarisasi gelombang P pada frontal plane
3. Aksis T : arah repolarisasi gelombang T pada frontal plane

Determining the Mean Electrical Axis (QRS axis)
Lead I : 4 – 0 = 4
Lead aVF : 12 – 2 = 10

Lead I : 4 – 0 = 4
Lead aVF : 12 – 2 = 10
I
aVF
+ = 90°
+ = 0°/360°- = 180°
- = 270°

Axis nomenclature Lead I Lead aVF
1. Normal axis (0 to +90 degrees) Positive Positive
2. Left axis deviation (-30 to -90) Also check lead II. To be true left axis deviation, it should also be down in lead II. If the QRS is upright in II, the axis is still normal (0 to -30).
Positive Negative
3. Right axis deviation (+90 to +180) Negative Positive
4. Indeterminate axis (-90 to -180) Negative Negative
Determining the Mean Electrical Axis (QRS axis)

Differential Diagnosis
Left axis deviation
LVH, left anterior fascicular block, inferior wall MI, PVC from the right ventricle, WPW syndrome activating the right ventricle, Pregnancy, Ascites, Abdominal tumor, exhalation.
Right axis deviation
RVH, left posterior fascicular block, lateral wall MI, PVC from the left ventricle, WPW syndrome activating the left ventricle, Emphysema, Inhalation
ARTI KLINIS AKSIS QRS

Hipertrofi Jantung :
1. Atrium : a. Atrium kiri
b. Atrium kanan
c. Biatrial
2. Ventrikel : a. Ventrikel kiri
b. Ventrikel kanan
c. Biventrikel

Pembesaran Atrium : (Morfologi Gel. P)
a. Hipertrofi atrium kiri
- lead II : Notched wide (> 3mm) gelombang P.
- V1 : defleksi terminal negatif bertambah
b. Hipertrofi atrium kanan
- lead II : Amplitudo gelombang P > 2.5mm.
- V1 : defleksi terminal negatif bertambah.
c. Biatrial : gabungan

P PulmonalMorfologi Gelombang P
P Mitral

Hipertrofi atrium kiri
Hipertrofi atrium kanan
Biatrial

2. Ventrikel : a. Ventrikel kiri
b. Ventrikel kanan
c. Biventrikel
•1. LVH: (Left ventricular hypertrophy). a. Gelombang S (terbesar) di V1 atau V2 (dlm mm) ditambah gelombang R (terbesar) di V5 atau V6 (dlm mm) > 35mm. ("voltage criteria“) b. Gelombang R > 12 mm di aVL (LVH is more likely with a "strain pattern" which is asymmetric T wave inversion in those leads showing LVH).
A. Ventrikel kiri
Summary :• S wave V1 or V2 or R wave V5 or V6
of 30mm or greater. • LAD• QRS duration upper limit of normal• Shift in the ST segment or T wave
(strain pattern) V5 and V6

L V H

B. Ventrikel kanan
Summary of Criteria for RVHRemember, again, that the electrocardiographic criteria for chamber enlarge-ment have both low sensitivity and specificity. In summary, these are thethings to look for when trying to diagnose RVH:1. R to S ratio of >1.0 in V1 or V22. RAD3. Normal QRS duration4. Strain pattern V1 or V2 and in limb leads with the tallest R wave
•RVH: (Right ventricular hypertrophy). Gelombang R > gelombang S di V1 dan Gelombang R menurun dari V1 sampai V6.

R V H
R > 7R’>SRAD.
ST-TChangesV1-2

C. Biventrikel
Merupakan gabungan kriteria RVH dan LVH
ARTI KLINIS HIPERTROFI JANTUNG :
1. Pembesaran atrium kanan : ASD, Ebstein anomali
2. Pembesaran atrium kiri : Mitral stenosis, Mitral regurgitasi
3. Hipertrofi ventrikel kiri : Hipertensi, Aortic stenosis, Aortic regurgitasi, Mitral regurgitasi, VSD, PDA
4. Hipertrofi ventrikel kanan : PPOK, ASD, Pulmonal stenosis

ST-T Segment (ISKEMIA & INFARK)

Progression of an Acute Myocardial Infarction
An acute MI is a continuum that extends from the normal state to a full infarction:
■ Ischemia—Lack of oxygen to the cardiac tissue, represented by ST segment depression, T wave inversion, or both■ Injury—An arterial occlusion with ischemia, represented by ST segment elevation■ Infarction—Death of tissue, represented by a pathological Q wave
Normal
Ischemia
Injury
Infarction


ST Segment

Ishemia – Injury - Infarct
Accurate ECG interpretation in a patient with chest pain is critical. Basically, there can be three types of problems - ischemia is a relative lack of blood supply (not yet an infarct), injury is acute damage occurring right now, and finally, infarct is an area of dead myocardium. It is important to realize that certain leads represent certain areas of the left ventricle; by noting which leads are involved, you can localize the process. The prognosis often varies depending on which area of the left ventricle is involved (i.e. anterior wall myocardial infarct generally has a worse prognosis than an inferior wall infarct).
V1-V2 anteroseptal wall
V3-V4 anterior wall
V5-V6 anterolateral wall
II, III, aVF inferior wall
I, aVL lateral wall
V1-V2posterior wall (reciprocal)

Terminologi morfologi QRS
qRs RsR
rS
QR Q/QS RsR’ rSr’

Irama Bukan Sinus/Arrytmia
• Atrial Fibrilasi :– Normo response (60-100 x/menit)– Rapid response ( > 100 x/menit)– Slow response ( < 60 x/menit)
• Atrial Flutter• SVT• VT• VF

•Atrial Fibrillation Many sites within the atria are generating their own electrical impulses, leading to irregular conduction of impulses to the ventricles that generate the heartbeat. This irregular rhythm can be felt when palpating a pulse. Looking at the ECG you'll see that:•Rhythm - Irregularly irregular •Rate - usually 100-160 beats per minute but slower if on medication •QRS Duration - Usually normal •P Wave - Not distinguishable as the atria are firing off all over •P-R Interval - Not measurable •The atria fire electrical impulses in an irregular fashion causing irregular heart rhythm
Note ectopic focus top right corner of atria.

•Atrial Flutter Looking at the ECG you'll see that:•Rhythm - Regular •Rate - Around 110 beats per minute •QRS Duration - Usually normal •P Wave - Replaced with multiple F (flutter) waves, usually at a ratio of 2:1 (2F - 1QRS) but sometimes 3:1 •P Wave rate - 300 beats per minute •P-R Interval - Not measurable •As with SVT the abnormal tissue generating the rapid heart rate is also in the atria, however, the atrioventricular node is not involved in this case.

•Supraventricular Tachycardia (SVT) AbnormalA narrow complex tachycardia or atrial tachycardia which originates in the 'atria' but is not under direct control from the SA node. SVT can occur in all age groupsLooking at the ECG you'll see that:•Rhythm - Regular •Rate - 140-220 beats per minute •QRS Duration - Usually normal •P Wave - Often buried in preceding T wave •P-R Interval - Depends on site of supraventricular pacemaker •Impulses stimulating the heart are not being generated by the sinus node, but instead are coming from a collection of tissue around and involving the atrioventricular (AV) node

PR Interval• Mulai dari awal gel. P sampai awal kompleks
QRS.• Nilai normal : 0,12 – 0,20’’ (3-5 kotak kecil)• Bila memanjang terjadi AV blok

•1st Degree AV Block1st Degree AV block is caused by a conduction delay through the AV node but all electrical signals reach the ventricles. This rarely causes any problems by itself and often trained athletes can be seen to have it. The normal P-R interval is between 0.12s to 0.20s in length, or 3-5 small squares on the ECG. Looking at the ECG you'll see that:•Rhythm - Regular •Rate - Normal •QRS Duration - Normal •P Wave - Ratio 1:1 •P Wave rate - Normal •P-R Interval - Prolonged (>5 small squares)

•2nd Degree Block Type 1 (Wenckebach)Another condition whereby a conduction block of some, but not all atrial beats getting through to the ventricles. There is progressive lengthening of the PR interval and then failure of conduction of an atrial beat, this is seen by a dropped QRS complex. Looking at the ECG you'll see that:•Rhythm - Regularly irregular •Rate - Normal or Slow •QRS Duration - Normal •P Wave - Ratio 1:1 for 2,3 or 4 cycles then 1:0. •P Wave rate - Normal but faster than QRS rate •P-R Interval - Progressive lengthening of P-R interval until a QRS complex is dropped

•2nd Degree Block Type 2 When electrical excitation sometimes fails to pass through the A-V node or bundle of His, this intermittent occurance is said to be called second degree heart block. Electrical conduction usually has a constant P-R interval, in the case of type 2 block atrial contractions are not regularly followed by ventricular contraction. Looking at the ECG you'll see that:•Rhythm - Regular •Rate - Normal or Slow •QRS Duration - Prolonged •P Wave - Ratio 2:1, 3:1 •P Wave rate - Normal but faster than QRS rate •P-R Interval - Normal or prolonged but constant

•3rd Degree Block3rd degree block or complete heart block occurs when atrial contractions are 'normal' but no electrical conduction is conveyed to the ventricles. The ventricles then generate their own signal through an 'escape mechanism' from a focus somewhere within the ventricle. The ventricular escape beats are usually 'slow'Looking at the ECG you'll see that:•Rhythm - Regular •Rate - Slow •QRS Duration - Prolonged •P Wave - Unrelated •P Wave rate - Normal but faster than QRS rate •P-R Interval - Variation •Complete AV block. No atrial impulses pass through the atrioventricular node and the ventricles generate their own rhythm

Durasi QRS
• Normal : < 0,12’’ (3 kotak kecil)
• Lebar sering terjadi pada RBBB dan LBBB.


Right bundle branch block


Left bundle branch block

Non Sustained Abnormal Beat/Arrytmia Ventrikel
• Premature Ventricular Contraction(PVC)/
Ventricular ExtraSystole (VES)
- Multifokal
- Couplet
- Bigemini or trigemini
• Ventricular Tachycardia
• Ventricular Fibrilation

Ventricle Extra Systole = Ventricle Premature Contraction

SR SR SR SRSR SR
VES VES
Sinus rhythm with Multifocal VES

Sinus rhythm with VES couplet



The Deadly
Rhythms
VT VFPEA
(Pulse less ElectricalActivity)
Asystole

•Ventricular Tachycardia (VT) AbnormalLooking at the ECG you'll see that:•Rhythm - Regular •Rate - 180-190 Beats per minute •QRS Duration - Prolonged •P Wave - Not seen •Results from abnormal tissues in the ventricles generating a rapid and irregular heart rhythm. Poor cardiac output is usually associated with this rhythm thus causing the pt to go into cardiac arrest. Shock this rhythm if the patient is unconscious and without a pulse

•Ventricular Fibrillation (VF) AbnormalDisorganised electrical signals cause the ventricles to quiver instead of contract in a rhythmic fashion. A patient will be unconscious as blood is not pumped to the brain. Immediate treatment by defibrillation is indicated. This condition may occur during or after a myocardial infarct.Looking at the ECG you'll see that:•Rhythm - Irregular •Rate - 300+, disorganised •QRS Duration - Not recognisable •P Wave - Not seen •This patient needs to be defibrillated!! QUICKLY


•Asystole - AbnormalLooking at the ECG you'll see that:•Rhythm - Flat •Rate - 0 Beats per minute •QRS Duration - None •P Wave - None •Carry out CPR!!

TERIMA KASIH

Prinsip pengukuran arus listrik pada jantung
- +
+
+
positive
negative
Bifasik
-
-

Patofisiologi Jantung
• Siklus Jantung


Torsade de Pointes







Diagnostic criteria for right bundle branch block1. QRS duration >0.12 s2. A secondary R wave (R’) in V1 or V23. Wide slurred S wave in leads I, V5, and V6Associated feature1. ST segment depression and T wave inversion
in the right precordial leads
RIGHT BUNDLE BRANCH BLOCK (RBBB)

Diagnostic criteria for left bundle branch block1. QRS duration of >0.12 s 2. Broad monophasic R wave in leads 1, V5, and V63. Absence of Q waves in leads V5 and V6Associated features1. Displacement of ST segment and T wave in an opposite direction to the
dominant deflection of the QRS complex (appropriatediscordance)2. Poor R wave progression in the chest leads3. RS complex, rather than monophasic complex, in leads V5 and V64. Left axis deviation—common but not invariable finding
LEFT BUNDLE BRANCH BLOCK (LBBB)

KRITERIA LAH :1. LAD, sering mendekati −60 derajat2. Gelombang R kecil di lead III3. Gelombang Q kecil di lead I4. Normal QRS durasi
LEFT ANTERIOR HEMIBLOCKS

KRITERIA LPH :1. RAD, sering mendekati +120 derajat2. Gelombang Q kecil di lead III3. Gelombang R kecil di lead I4. Normal QRS durasi
LEFT POSTERIOR HEMIBLOCKS

BUNDLE BRANCH BLOCK :1. KOMPLIT : - kanan : RIGHT BUNDLE BRANCH BLOCK (>0,12”) - kiri : LEFT BUNDLE BRANCH BLOCK
2. INKOMPLIT : - kanan : INCOMPLETE RIGHT BUNDLE BRANCH BLOCK
(<0,12”) - kiri : INCOMPLETE LEFT BUNDLE BRANCH BLOCK
1. RIGHT BUNDLE BRANCH BLOCK (RBBB)
2. LEFT BUNDLE BRANCH BLOCK (LBBB)
3. LEFT ANTERIOR HEMI BLOCK (LAH)
4. LEFT POSTERIOR HEMI BLOCK (LPH)
INTRAVENTRICULAR CONDUCTION DELAY

Dextroposisi dan Dextrocardia
Normal

Dextroversi / Dextroposisi

Dextrocardia

Cara membedakan normal/dextroposisi dengan dextrocardia
Normal Dextrocardia
LA-RA I -I
LL-RA II III
LL-LA III II
aVR aVL
aVL aVR
aVF aVF

Normal Dextrocardia
LA-RA I -I
LL-RA II III
LL-LA III II
aVR aVL
aVL aVR
aVF aVF
Related Documents