DASAR – DASAR KEMOTERAPI DASAR – DASAR KEMOTERAPI PADA PENDERITA KANKER PADA PENDERITA KANKER PELATIHAN SINGKAT TATALAKSANA KEMOTERAPI PELATIHAN SINGKAT TATALAKSANA KEMOTERAPI PADA PENDERITA KANKER PADA PENDERITA KANKER BAGI TENAGA PARAMEDIS / PERAWAT RUMAH BAGI TENAGA PARAMEDIS / PERAWAT RUMAH SAKIT SANGLAH DENPASAR, 15 APRIL 2006 SAKIT SANGLAH DENPASAR, 15 APRIL 2006

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

DASAR – DASAR KEMOTERAPI DASAR – DASAR KEMOTERAPI PADA PENDERITA KANKERPADA PENDERITA KANKER
PELATIHAN SINGKAT TATALAKSANA KEMOTERAPI PELATIHAN SINGKAT TATALAKSANA KEMOTERAPI PADA PENDERITA KANKER PADA PENDERITA KANKER
BAGI TENAGA PARAMEDIS / PERAWAT RUMAH BAGI TENAGA PARAMEDIS / PERAWAT RUMAH SAKIT SANGLAH DENPASAR, 15 APRIL 2006 SAKIT SANGLAH DENPASAR, 15 APRIL 2006

PENDAHULUANPENDAHULUAN
MODALITAS TERAPI KANKER:MODALITAS TERAPI KANKER:
BEDAHBEDAHRADIAOTERAPIRADIAOTERAPIKEMOTERAPIKEMOTERAPITERAPI HORMONALTERAPI HORMONAL
TERAPI GENTERAPI GEN
TERAPI IMUNOLOGITERAPI IMUNOLOGI

PedahuluanPedahuluan
KEMOTERAPIKEMOTERAPI
BAGIAN INTEGRAL PENANGANAN KANKER. BAGIAN INTEGRAL PENANGANAN KANKER.
BAHAN KIMIA YG DAPAT MENGHAMBAT BAHAN KIMIA YG DAPAT MENGHAMBAT PERTUMBUHAN SEL PERTUMBUHAN SEL
KANKER.KANKER.
OBAT KERASOBAT KERAS
TATALAKSANA KHUSUSTATALAKSANA KHUSUS
PERLU PENGETAHUAN, KETERAMPILAN YANG PERLU PENGETAHUAN, KETERAMPILAN YANG MEMADAIMEMADAI

TUJUAN PEMBERIAN KEMOTERAPITUJUAN PEMBERIAN KEMOTERAPIMencapai kesembuhan (kuratif)Mencapai kesembuhan (kuratif)Mempepanjang masa bebas penyakit Mempepanjang masa bebas penyakit (DFS).(DFS).Memperpanjang lama hidup (Survival)Memperpanjang lama hidup (Survival)Memperbaiki kualitas hidup (QoL)Memperbaiki kualitas hidup (QoL)
SEBAGAI: AdjuvantSEBAGAI: Adjuvant Neoadjuvant Neoadjuvant Terapi utama Terapi utama Radiosensitizer Radiosensitizer

PRINSIP DASARPRINSIP DASAR
ASPEK ONKOLOGIASPEK ONKOLOGI ASPEK PENDERITA DAN KELUARGAASPEK PENDERITA DAN KELUARGA HASIL PENGOBATAN DAN EFEK HASIL PENGOBATAN DAN EFEK
SAMPINGSAMPING

ASPEK ONKOLOGIASPEK ONKOLOGI
Diagnosis kanker:Diagnosis kanker:Klinis, Imaging, Patologi. Klinis, Imaging, Patologi.
Marker Marker Biologi.Biologi. Stadium kankerStadium kanker Performance status (Karnofski, Performance status (Karnofski,
ECOG,WHO). ECOG,WHO). faktor risikofaktor risiko

Aspek penderita dan Aspek penderita dan keluagakeluaga
INFORMASI MENGENAI:INFORMASI MENGENAI:IndikasiIndikasiJenis, cara, siklus, lama pemberian Jenis, cara, siklus, lama pemberian
obatobat
Efek sampingEfek samping
Informed consentInformed consent
Hasil terapi dan efek Hasil terapi dan efek sampingsamping
Hasil terapi sesuai dengan tujuan Hasil terapi sesuai dengan tujuan pengobatanpengobatan
Efek samping:Efek samping:diagnosisdiagnosispenangananpenanganan

KEMOTERAPI YANG BAIKKEMOTERAPI YANG BAIK EFEKTIFEFEKTIF AMANAMAN SPESIFIKSPESIFIK SELEKTIFSELEKTIF
CARA KERJA KEMOTERAPICARA KERJA KEMOTERAPI
BEKERJA PADA SEL YANG SANGAT AKTIFBEKERJA PADA SEL YANG SANGAT AKTIF DOSIS MAKSIMUM YANG DITOLERANSIDOSIS MAKSIMUM YANG DITOLERANSI Tingkat seluler:Tingkat seluler:
Sel proliferasiSel proliferasiSiklus selSiklus selApoptosisApoptosis
Fase spesifik atau non spesifikFase spesifik atau non spesifik Cara pemberian :IV, Oral, instilasi, perfusiCara pemberian :IV, Oral, instilasi, perfusi Terapi tunggal atau kombinasiTerapi tunggal atau kombinasi

DNA replicationP33 cdc2Cyclin A
S
G1
M
G2
Mitosis/MiosisP34 cdc2 Cyclin B
MAP kinase
G2 controlP34cdc2 cyclin A& B
MAP kinase
Start/Restriction pointG1 ControlP33 cdc7, p34 cdc4, p33cdc6
Cyclin E & D
P53Synthesis enzyme for DNA
Taxan : microtubulin, m’blok mitosis dg m’aktivasi p34 cdc2
Doxo : merangsang p53

MG2
G1S
Bleomycin
5 Fudrara C6-Hydroxyurea
5 FUMETHOTREXATE
6-Thioguanine
6-Marcaptopurine
Mytomycin
Actinomycin D
Hydrocortisone Chalones
5 FU
VinblastineVincristineColchicineGriseofulvin
Differentiation
Phleomycin
Cyclophosphamide
Purin antagonis
Hydroxy urea
Actinomycin
Cyclophosphamide
5 Fudr .5FU, Ara C. Mitomycin,Doxorubicin Thioguanine
18-30h6-20h
0,5-1h
0.5-1h
2-10h
Doxorubicin
Alkylating agent, Antimetabolit,Mitotic inhibitor, Antibiotic

No response Early recurrence Late recurrence
Tumor detectable(clinically)
Long-term Remission Not palpable
Immune resistanceof host
(humoral&cellular)
Induction Consolidation Maintenance Cure
1012
109
106
103
(1kg)
(1 g)
(1 mg)
Number ofTumor cell
Tumor invisible(Remission)
(1 úg)

1.Objective Response Evaluation2.Subjective Response Evaluation(3). Survival
CANCER TREATMENT OUTCOME

OBJECTIVE RESPONSE EVALUATIONS
1. TUMOR SIZE : - Complete remission (CR) - Partial remission (PR) - No Changes (Stable Disease = St D) - Progressive Disease (PD)
2. Marker Tumour : - CEA, CA15-3, MCA Breast Ca - CEA, CA19-9 Pancreas Ca, Colorectal Ca - HCG Chorio Ca - PSA Prostat Ca
3. Objective-Qualitative : - Change of Clinical sign : Brain Ca-neurology sign
SUBJECTIVE RESPONSE EVALUATION
Performance status : Karnofsky / ECOG
Palliative
CURATIVE : caution of safety and side effects

DIAGNOSE of Side Effect
PHARMACOLOGYWhen Side effect become: NADIR point (degree of SE)Onset of SE, Specificity of organ target
MANAGEMENT of Side Effect
Anticipation & PreventionDose related side effect monitoringEarly treatment of side effect
SIDE EFFECT MONITORING

1. Onset of SE : - Immediately ( < 1 Hour post Chemotx) Anaphylaxsis - early (1- 48 hours ) Nausea-Vomiting profuse - delayed (2 days -2 months ) leucopenia - Late (after 2 months ) myopathy, neuropathy
2.Organ Target : Haematologic, Skin, Cardiovascular, Respiratory, Gastrointestinal, CNS.
3.Level/degree of SE (IUCC,WHO, ECOG) : - grade 0-2 : tolerable ( safety enough ) - grade 3 (severe) : must be alert (Yellow light), need treatment ± - grade 4 (life threatening) : Hazard, early and adequate treatment

PROFILE EPISODE of FEBRIL NEUTROPENI
Chemotherapy day
Chemotherapy day
nadir1 6 11 16 21 26

FEBRILE NEUTROPENIAFEBRILE NEUTROPENIA
CRITERIA :
• NEUTROPENIA :
absolute count of neutrophill in circulating blood < 2000 cells/mm3
• FEVER :
body temperature > 38.50C in 3 x measurement per 24 hours
CRITERIA :
• NEUTROPENIA :
absolute count of neutrophill in circulating blood < 2000 cells/mm3
• FEVER :
body temperature > 38.50C in 3 x measurement per 24 hours
DEGREE OF NEUTROPENIADEGREE OF NEUTROPENIA
• Mild : 2000 – 1000 cells/mm3• Moderate : 1000 – 500 cells/mm3• Severe : < 500 cells/mm3
• Mild : 2000 – 1000 cells/mm3• Moderate : 1000 – 500 cells/mm3• Severe : < 500 cells/mm3

TREATMENT of FEBRIL NEUTROPENI
Empiric antibacterial
Empiric antibacterial
Chemotherapy day
Chemotherapy day
nadir
G-CSFSterile room



Hiperpigmentation (Fluorouracil )

Management Side Effect
1. ANTIDOTUM to specific agent : - Antidotum of MTX : Calcium leucovorin, Ca Lefofolinat - Cardiomyopathy prophylaxis – Doxorubicin > 450 mg/m2 * Dexrazosane 10 mg – Doxorubicin 1 mg
2. Dose modification : - Toxicity grade 3 and 4 : decrease dose 25% - 50%
3. Supportive Drugs : - Haemopoetic GF : G-CSF, GM-SF, IL-3, Epo - Component Blood transfuse - Selective antibiotic
4. Sterile Room technology
Three types of CINV: Three types of CINV:
Acute nausea vomiting (12-24h)Acute nausea vomiting (12-24h) Delayed nausea vomiting (up to 5 Delayed nausea vomiting (up to 5
days)days) Anticipatory nausea vomiting (result Anticipatory nausea vomiting (result
from patient’s expectation from patient’s expectation (anticipation) of NV.(anticipation) of NV.

Risk factors for CINV:Risk factors for CINV:
Patients risk factors:Patients risk factors:AgeAgeGenderGenderHistory of NVHistory of NVHistory of alcohol use.History of alcohol use.
Drug risk factors (see table)Drug risk factors (see table) Procedural risk factors (RINV).Procedural risk factors (RINV).
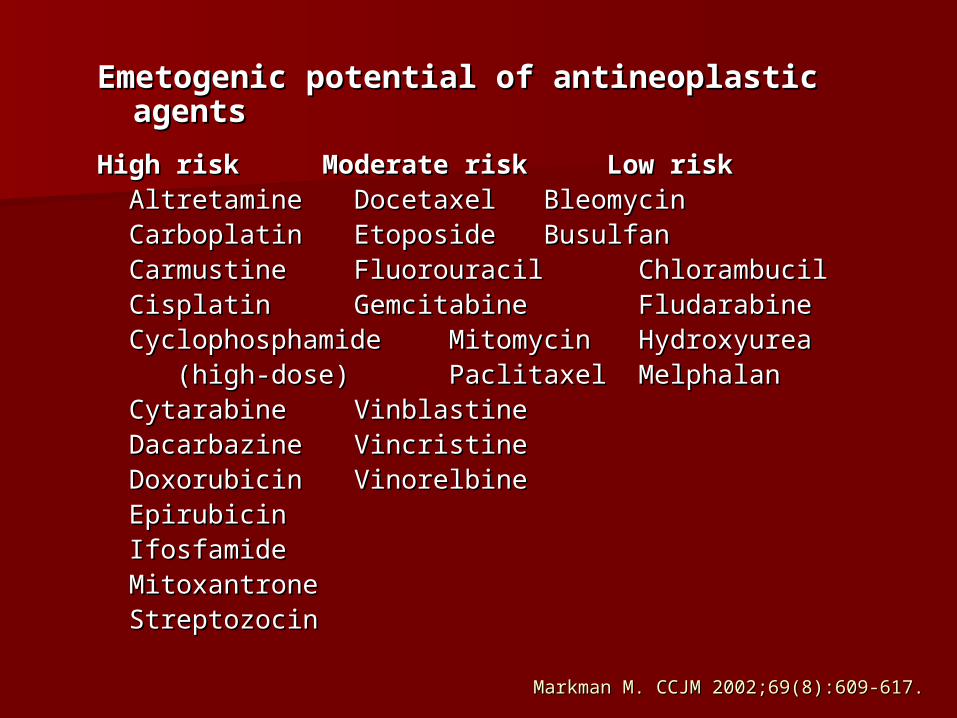
Markman M. CCJM 2002;69(8):609-617.Markman M. CCJM 2002;69(8):609-617.
Emetogenic potential of antineoplastic agents Emetogenic potential of antineoplastic agents
High risk High risk Moderate riskModerate risk Low riskLow risk Altretamine Altretamine Docetaxel Docetaxel Bleomycin Bleomycin CarboplatinCarboplatin Etoposide Etoposide Busulfan Busulfan Carmustine Carmustine Fluorouracil Fluorouracil Chlorambucil Chlorambucil Cisplatin Cisplatin Gemcitabine Gemcitabine
Fludarabine Fludarabine Cyclophosphamide Cyclophosphamide Mitomycin Mitomycin Hydroxyurea Hydroxyurea (high-dose)(high-dose) Paclitaxel Paclitaxel Melphalan Melphalan Cytarabine Cytarabine Vinblastine Vinblastine Dacarbazine Dacarbazine Vincristine Vincristine Doxorubicin Doxorubicin Vinorelbine Vinorelbine Epirubicin Epirubicin Ifosfamide Ifosfamide MitoxantroneMitoxantrone Streptozocin Streptozocin

Hesketh PJ, Kris MG, Grunberg SM, et al. J Clin Oncol. 1997;15:103-109Hesketh PJ, Kris MG, Grunberg SM, et al. J Clin Oncol. 1997;15:103-109
Emetogenic Potential of Single Chemotherapy AgentsEmetogenic Potential of Single Chemotherapy Agents
LeveLevell
Frequency of Frequency of Emesis (%)Emesis (%)
Chemotherapeutic Chemotherapeutic
AgentsAgents
55 > 90> 90 Carmustine > 250 mg/mCarmustine > 250 mg/m22
Cisplatin >=50 mg/mCisplatin >=50 mg/m22
Cyclophosphamide >1,500 mg/mCyclophosphamide >1,500 mg/m22
Dacarbazine Dacarbazine
Mechlorethamine Mechlorethamine
Streptozocin Streptozocin
44 60 – 9060 – 90 Carboplatin Carboplatin
Carmustine <=250 mg/mCarmustine <=250 mg/m22
Cisplatin <50Cisplatin <50 mg/mmg/m22
Cyclophosphamide >750 mg/mCyclophosphamide >750 mg/m22 <=1,500 mg/m <=1,500 mg/m22
Cytarabine >1 g/mCytarabine >1 g/m22
Doxorubicin >60 mg/mDoxorubicin >60 mg/m22
Methotrexate >1,000 mg/mMethotrexate >1,000 mg/m22
Procarbazine (oral)Procarbazine (oral)
33 30 – 6030 – 60 Cyclophosphamide >=750 mg/mCyclophosphamide >=750 mg/m22
Cyclophosphamide (oral)Cyclophosphamide (oral)
Doxorubicin 20-60 mg/mDoxorubicin 20-60 mg/m22
Epirubicin <=90 mg/mEpirubicin <=90 mg/m22
Hexamethylmelamine (Oral)Hexamethylmelamine (Oral)
Idarubicin Idarubicin
IfosfamideIfosfamide
Methotrexate 250-1,000 mg/mMethotrexate 250-1,000 mg/m22
Mitoxantrone <15 mg/mMitoxantrone <15 mg/m22
22 10 – 3010 – 30 DocetaxelDocetaxel
EtoposideEtoposide
5-Fluorouracil >1,000 mg/m5-Fluorouracil >1,000 mg/m22
Gemcitabine Gemcitabine
Methotrexate >50 mg/mMethotrexate >50 mg/m22 to <250 mg/m to <250 mg/m22
MitomycinMitomycin
PaclitaxelPaclitaxel
11 < 10< 10 Bleomycin Bleomycin
Busulfan Busulfan
Chlorambucil (oral)Chlorambucil (oral)
2-Chlorodexyadenosine2-Chlorodexyadenosine
FludarabineFludarabine
HydroxyureaHydroxyurea
Methotrexate <=50 mg/mMethotrexate <=50 mg/m22
L-phenylalanine mustard (oral)L-phenylalanine mustard (oral)
Thioguanine (oral)Thioguanine (oral)
Vinblastine Vinblastine
VincristineVincristine
VinorelbineVinorelbine

The neuronal pathway of The neuronal pathway of CINVCINV
Vomiting center in the medulla (lateral Vomiting center in the medulla (lateral reticular formation)reticular formation)
Chemoreceptor Trigger Zone (CTZ) Chemoreceptor Trigger Zone (CTZ) area prostrema 4area prostrema 4thth ventricle. ventricle.
Neurotransmitters: dopamin, Neurotransmitters: dopamin, serotonin, neurokinin and their serotonin, neurokinin and their receptors.receptors.
Nuroreceptors in Enterochromaffin cell Nuroreceptors in Enterochromaffin cell GI tract.GI tract.

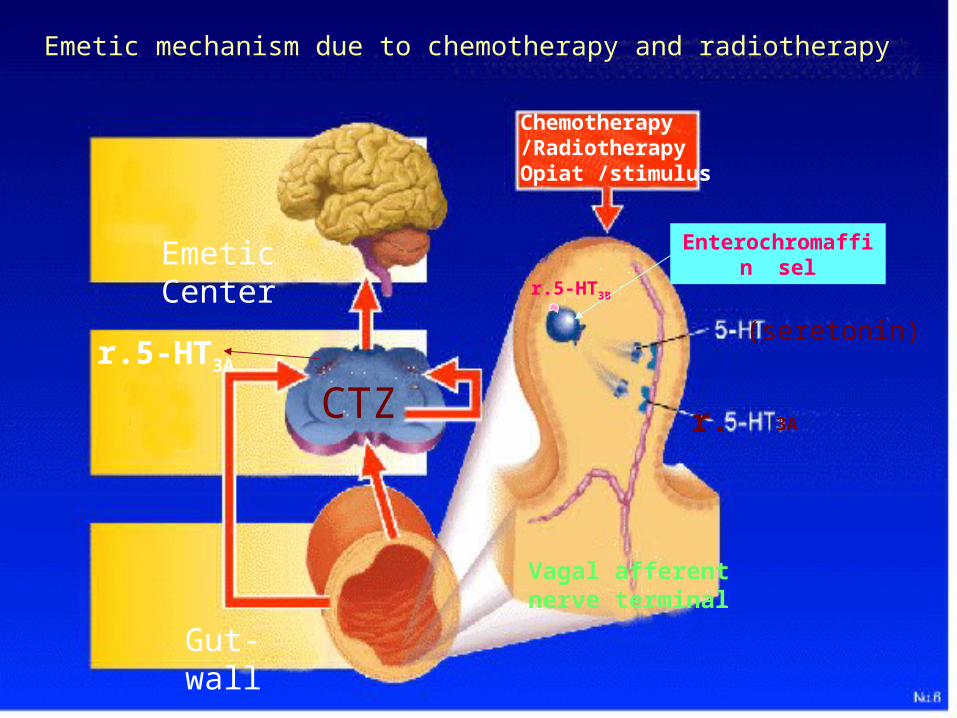
Enterochromaffin sel
3ACTZ
Gut-wall
Emetic Center
Emetic mechanism due to chemotherapy and radiotherapy
Vagal afferent nerve terminal
(seretonin)r.5-HT3A
Chemotherapy/RadiotherapyOpiat /stimulus
r.5-HT3B
r.

Emetogenic stimulus
ondansetron

Complication of CINVComplication of CINV
DehydrationDehydration Electrolyte imbalanceElectrolyte imbalance Aspiration pneumoniaAspiration pneumonia Very distressing for patients Very distressing for patients
choosing discontinue potentially choosing discontinue potentially curative therapy.curative therapy.
Economic burdenEconomic burden

Treatment of CINVTreatment of CINV
Preventing CINV is more effective Preventing CINV is more effective than treating itthan treating it
Anti emetic drugs:Anti emetic drugs:Serotonin-receptor antagonist Serotonin-receptor antagonist
(5-HT3 (5-HT3 receptor antagonist).receptor antagonist).CorticosteroidCorticosteroidOthersOthers
corticosteroids potentiate seretonin-corticosteroids potentiate seretonin-receptor antagonist.receptor antagonist.


Serotonin-receptor antagonistsSerotonin-receptor antagonists
DRUGDRUG DOSAGE DOSAGE
Dolasetron Dolasetron 100 mg IV (single dose)100 mg IV (single dose)
100 mg orally (single dose)100 mg orally (single dose)
Granisetron Granisetron 1-2 mg IV (single dose)1-2 mg IV (single dose)
1 or 2 mg orally (single dose)1 or 2 mg orally (single dose)
OndansetronOndansetron 8 mg IV (single dose)8 mg IV (single dose)
16-24 mg orally (single dose)16-24 mg orally (single dose)
or 8 mg orally twice daily or 8 mg orally twice daily
Others (Tropisetron, Itasetron)Others (Tropisetron, Itasetron)
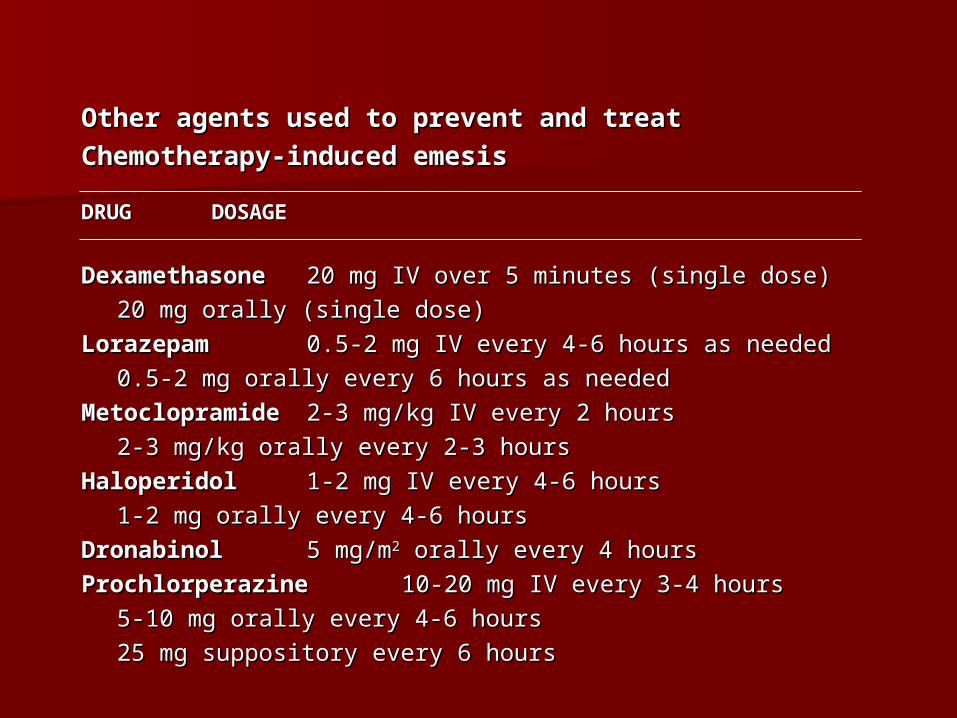
Other agents used to prevent and treatOther agents used to prevent and treat
Chemotherapy-induced emesisChemotherapy-induced emesis
DRUGDRUG DOSAGE DOSAGE
Dexamethasone Dexamethasone 20 mg IV over 5 minutes (single dose)20 mg IV over 5 minutes (single dose)
20 mg orally (single dose)20 mg orally (single dose)
Lorazepam Lorazepam 0.5-2 mg IV every 4-6 hours as needed0.5-2 mg IV every 4-6 hours as needed
0.5-2 mg orally every 6 hours as 0.5-2 mg orally every 6 hours as neededneeded
MetoclopramideMetoclopramide 2-3 mg/kg IV every 2 hours2-3 mg/kg IV every 2 hours
2-3 mg/kg orally every 2-3 hours 2-3 mg/kg orally every 2-3 hours
Haloperidol Haloperidol 1-2 mg IV every 4-6 hours 1-2 mg IV every 4-6 hours
1-2 mg orally every 4-6 hours1-2 mg orally every 4-6 hours
DronabinolDronabinol 5 mg/m5 mg/m22 orally every 4 hours orally every 4 hours
Prochlorperazine Prochlorperazine 10-20 mg IV every 3-4 hours 10-20 mg IV every 3-4 hours
5-10 mg orally every 4-6 hours 5-10 mg orally every 4-6 hours
25 mg suppository every 6 hours 25 mg suppository every 6 hours
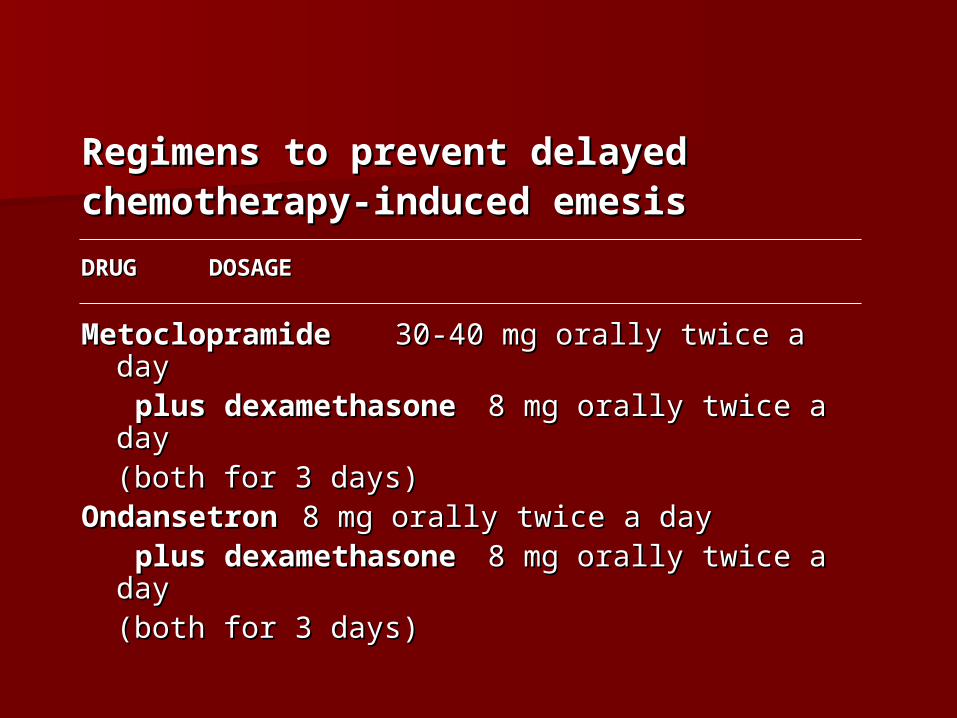
Regimens to prevent delayedRegimens to prevent delayedchemotherapy-induced emesischemotherapy-induced emesis
DRUGDRUG DOSAGE DOSAGE
Metoclopramide Metoclopramide 30-40 mg orally twice a 30-40 mg orally twice a day day
plus dexamethasoneplus dexamethasone 8 mg orally twice a day 8 mg orally twice a day (both for 3 days)(both for 3 days)
Ondansetron Ondansetron 8 mg orally twice a day 8 mg orally twice a day plus dexamethasoneplus dexamethasone 8 mg orally twice a day 8 mg orally twice a day
(both for 3 days)(both for 3 days)

Tepat indikasi : kemoterapi tepat dipilih berdasar titik tangkap kerjanya berdasar patogenesis kanker sehingga dapat tercapai tujuan : 1.kuratif 2.mencapai bebas penyakit (DFS) yang lebih lama 3.neoadjuvant (Mikrometastasis,mengecilkan volume tumor preoperasi-down staging) 4.mempertahankan atau meningkatkan quality of life (terapi paliatif)

Tepat cara pemberian obat : oral, IV, bolus, infusion dsb yang penting : penderita nyaman , tidak takut dan dengan kesadaran sendiri ingin melanjutkan kemoterapi Tepat monitoring efek obat : - penilaian hasil / respons terapi - kemampuan hidup (quality of life) dan - efek samping obat
Tepat jenis obat : sebaiknya lebih spesifik, selektif, mem- punyai Response rate tinggi, established, dan dapat dijangkau oleh penderita
Tepat dosis obat : sesuai Maximum Tolerated Dose ( Risk group )
TERIMAKASIHSEMOGA BERMANFAAT
Related Documents











