PATOGENESIS,DIAGNOSIS DAN PENG ELOLAAN MEDIK HEMORROID H.Ali Djumhana SubBag.Gastroenterohepatologi - SMF/Bagian Ilmu Penyakit Dala m Rumah Sakit UmumPusat Dr Hasan Sadikin - Fakultas Kedokteran Unpad Ban dung Abstrak Hemorroid merupakan penyakit y ang cuku p sering terjadi,walaupun pato genesisnya belum sepenuhnya difahami tetapi per anan kerusakan penyangga pembu luh darah,hipertrofi sfinkter ani dan beberapa fakt or pemburuk yang menyebabkan p eningkatan tekanan intrarektum mempunyai kontribu si untuk terjadinya hemorroid.Lingkaran setan ber upa protrusi pleksus hemorroid yan g akan meningkatkan tekanan sf inkter ani kemudian menambah kongesti aliran darah dan menambah besar hemorroid. Tujuan terapi untuk mengurangi kongesti pembuluh d arah,fiksasi mukosa pada lapis an otot dan mengurangi ukuran dan jumlah pleksus hemo rroidalis.Terapi medik diberik an terbatas pada hemorroid grade 1 dan 2.Terapi medik non farmakologik dengan mengatur d

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PATOGENESIS,DIAGNOSIS DAN PENGELOLAAN MEDIK HEMORROIDH.Ali DjumhanaSubBag.Gastroenterohepatologi -SMF/Bagian Ilmu Penyakit Dalam Rumah Sakit UmumPusat Dr HasanSadikin -Fakultas Kedokteran Unpad BandungAbstrakHemorroid merupakan penyakit yang cukup sering terjadi,walaupun patogenesisnya belum sepenuhnya difahami tetapi peranan kerusakan penyangga pembuluh darah,hipertrofi sfinkter ani dan beberapa faktor pemburuk yang menyebabkan peningkatan tekanan intrarektum mempunyai kontribusi untuk terjadinyahemorroid.Lingkaran setan berupa protrusi pleksus hemorroid yang akan meningkatkan tekanan sfinkter ani kemudian menambah kongesti aliran darahdan menambah besar hemorroid.Tujuan terapi untuk mengurangi kongesti pembuluh darah,fiksasi mukosa pada lapisanotot dan mengurangi ukuran dan jumlah pleksus hemorroidalis.Terapi medik diberikan terbatas pada hemorroid grade 1 dan 2.Terapi medik nonfarmakologik dengan mengatur diit dan kebiasaan defekasi,pemberian supplemenserat dan pelunak feses.Obat steroid topikal sebagai antiinflammasi dapat diberikanpada fase akut,obat flebotonik dapat diberikan pada fase

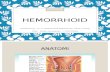
akut dan kronik.Terapi minimalinvasip dengan skleroterapi,ligasi, bedah krio,dilatasi anus dan koagulasi.Untuk hemorroid yang telah lanjut perlu dilakukan terapi bedah .PendahuluanHemorroid adalah penyakit yangcukup sering terjadi di masyarakat dan tersebar luas diseluruh dunia.Prevalensi penyakit ini di USA diperkirakansekitar 4-5%(1).Hemorroid bukan penyakit yang fatal,tetapi sangat mengganggu kehidupan.Sebelumnya hemorroid ini dikira hanya timbul karena stasis aliran darah daerah pleksus hemorroidalis,tetapi ternyata tidak sesederhana itu.Simptomatologi sering tidak sejalan dengan besarnya hemorroid ,kadang-kadang hemoroid yang besar tidak/hanya sedikit memberikan keluhan, sebaliknya hemorroid kecil dapat memberikan gejala perdarahan masip(1,2,3,4).Karena itu untuk diagnosis hemorroid memerlukananamnesis,pemeriksaan fisik dan pemeriksaan konfirmasi yang teliti serta perlu dievaluasi dengan seksama agar dapat dicapai pendekatan terapeutik yang sesuai.PatogenesisPleksus hemorroidalis merupakan sistem artereriovenous anastomosisyang terletak

didaerah submukosa kanalis analis.Terdapat dua buah pleksus yaitu pleksus hemorroidalis internal dan eksternal yang terpisah satu denganyang lainnya,sebagai batas adalah linea dentata.Ada3 hal yang penting untuk diketahui,yaitu pertama adalah mukosa rektum atau mukosa anodermal,kemudian stroma jaringanyang berisi pembuluh darah,otot polos dan jaringan ikat penunjang serta ketiga adalah jangkar(anchor) yang akan melindungi pleksus hemorroid dari mekanisme kerja sfinkter ani.Dengan bertambah usia dan berbagai faktor pemburuk (seperti bendungan sistim porta,kehamilan,PPOK,konstipasi kronik,keadaanyang menimbulkan tekanan intrapelvis meningkat) )maka jaringan penunjang dan jangkar tersebut dapat menjadi rusak akibatnya pleksus akan menonjoldan turun dan memberikan simptom(1,2,).Teorilain menyatakan bahwa hemorroid ini mirip dengan suatu AV malformation,ini dibuktikan dengan adanya perdarahan yang berwarna merah(bukan hitam) seperti perdarahan arterial.Teori terakir menyatakan bahwa defek utama merupakan kombinasi dari lemahnya jaringan penyokong pleksushemorroidalis -hipertrofi dari otot sfinkter ani.Padabeberapa individu sfinkter ani interna hipertrofi sehingga kanalis

analis makin menyempit,pada saat mengedan terjadi kongesti,bolus feses menekan pleksus kebawah melalui sfinkter yang hipertrofi,terjadi kongesti dan menjadi simptomatik(3,4). Dalam hal iniakan terjadi sirkulus vitiosus yaitu;Penonjolan pleksus submukosa akan menimbulkan kanalis analis menjadi kaku hal ini merangsang sfinkter menjadi lebih kencang sehingga kongesti aliran darah menjadi semakin berat dan akhirnya penonjolan semakin besar(4,5).Tidak ada bukti bahwa keturunan dan faktor geografi turut berperan(4).Upaya pengobatan sebaiknya berdasarkan pada pendekatan bagaimana memotong lingkaran setan tadi.Diagnosis.Sebagian besar penderita mengeluh adanya perdarahan perrektal,perdarahan berrupa darah merah segar,menetes sewaktu atau setelah buang air besar.Perdarahan ini tidak disertai rasa nyeri atau rasa mules.Pada sebagian penderita perdarahan ini tidak diketahui,sehingga tidak jarang pasen dengan hemorroid ini datang dengan keluhan anemia.Sebagian lagi penderita mengeluh rasa nyeri.Rasa nyeri ini timbul bila ada trombosis atau strangulasi dari hemorroid.Sebagian kasus mungkin mengeluh adanya benjolan pada anusnya,atau adayang keluar(prolaps) dari anusnya.Keluhan lain mungkin

berupa pruritus ani,atau rasa tidak enak daerah anus atau ada discharge.Kadang-kadang hemorroid ditemukan secara kebetulan(asimptomatik)(1,2,3,4,5)Terhadap penderita dengan keluhan seperti diatas hendaknya dilakukan pemeriksaan fisik yang cermat. Penderita hemorroid derajat 3 dan 4 dengan mudah dapat dilihat pada saat pemeriksaan, pada hemorroid derajat 2 pasen perlu disuruh mengejan beberapa saat.Harus dilakukan colok dubur,anoskopi bahkan bila dianggap perlu(pada kasus perdarahan masip) dapat dilakukan colon inloop, rektosigmoidoskopi atau kolonoskopi untuk menyingkirkan penyakit lainseperti malgnansi kolorektal atau inflammatory bowel diseases.Pada beberapa senter dilakukan pemeriksaan tekanan sfinkter ani(4)Secara fisik beratnya hemorroid interna dibagi menjadi 4 derajat(grade)Grade 1Hemorroid terbatas pada lumen anorektal,tidak menonjol keluarGrade 2Hemorroid menonjol keluar saatmengedan dan masuk secara spontanGrade 3Hemorroid menonjol keluar dan harus didorong untuk memasukkannyaGrade 4Hemorroid menonjol dan tidak dapat masuk walaupun didorong.

Lokasi hemorroid interna yaitulateral kiri,lateroventral kanan dan laterodorsal kanan.TerapiTujuan terapi yaitu memotong lingkaran patogenesis hemorroiddengan berbagai cara:1.Mengurangi kongesti:-manipulasi diit dan mengatur kebiasaan-obat antiinflammasi-obat flebotonik-dilatasi anus-sfinkterotomi2.Fiksasi mukosa pada lapisan otot:+ skleroterapi+ koagulasi infra merah+ diatermi bipolar3.Mengurangi ukuran/vaskularisasi dari pleksus hemorroidalis: = ligasi= eksisiTerapi medikTerapi medik diberikan pada penderita hemorroid derajat 1 atau 2 (1,2,3,4,5).Manipulasi diit dan mengatur kebiasaan.Diit tinggi serat,bila perlu diberikan supplemen serat,atau obat yang memperlunak feses(bulkforming cathartic).Menghindarkan mengedan berlama-lama pada saat defekasi.Menghindarkan diare karena akan menimbulkan iritasi mukosa yang mungkin menimbulkan ekaserbasi penyakit.Obat antiinflammasi seperti steroid topikal jangka pendek d

apat diberikanuntuk mengurangi udem jaringan karena inflammasi.Antiinflammasi ini biasanya digabungkan dengan anestesi lokal,vasokonstriktor,lubricant,emollient dan zat pembersih perianal.Obat-obat ini tidak akan berpengaruh terhadap hemorroidnya sendiri,tetapi akan mengurangi inflammasi,rasa nyeri/tidak enak dan rasa gatal.Penggunaan steroid ini bermanfaat pada saat ekaserbasi akut dari hemorroid karena bekerja sebagai antiinflammasi,antipruritus dan vasokonstriktor.Walaupun demikian pemakaian jangka panjang malah menjadi tidak baik karena menimbulkan atrofikulit perianal yang merupakanpredisposisi terjadinya infeksi.Demikian pula obat yang mengandung anestesi lokal perlu diberikan secara hati-hati karena sering menimbulkanreaksi buruk terhadap kulit/mukosa.Sitz bath ( bagian anus direndam di waskom/ember dengan air hangat + permanganas kalikus) sangat bermanfaat karena ada efek memberiesihkan perianal.Obat flebotonik seperti Daflonatau preparat rutacea dapat meningkatkan tonus vena sehingga mengurangi kongesti.Daflon merupakan obat yang dapat meningkatkan dan memperlama efek noradrenalin pada pembuluh darah.Penelitian double blind placebo-

controlled dari Daflon ternyata memberikan manfaat untuk terapi hemorroid baik pada keadaan non akut maupun pada saat ekaserbasi akut.Dosis pada saat akut yaitu 3 x 1000 mg selama 4 hari dilanjutkan 2x 1000 mg selama 3 hari(6).Ternyata pengobatan dengan cara tersebut lebih baik dari plasebo.Penelitian lain pada hemorroid non akut dengan dosis 2 x 500 mg selama 2 bulan hasilnya kelompok yang diobati lebih baik dari plasebo(7). Obat ini dikatakanaman bahkan pada wanita hamilsekalipun(8).Terapi dengan cara "minimal invasive"Terapi dengan cara ini dlakukan terhadap penderita yang tidak berhasil dengan cara medik atau penderita yang belum mau dilakukan operasi.Paling optimal cara ini dilakukan pada penderita hemorroid derajat 2 atau 3.(1,2,3,4,5)Skleroterapi:Cara ini sudah sangat lama digunakan.Sklerosant(morhuat,etoksisklerol dsb) disuntikkan para varises sehingga terjadi inflammasi dan sklerosis lapisan submukosa.Cara ini bermanfaat untuk mengatasi hemorroid kecil yang sedang berdarah.Rubber band ligation:Dengan memakai aplikator khusus,hemorroid dihisap kemudian rubber band dilepaskan dan hemorroid terikat.Keadaan ini akan menimbulkan nekrosis lokal dan terjadi fibrosis serta fiksasi mukosa pada lapi

san otot.Dilatasi anusprosedur sangat simpel bisa dengan lokal anestesi atau neuroleptik.Bedah krio:Sebagiann dari mukosa anus dibekukan dengan nitrogen cair,dalam beberapa hari terjadi nekrosis,kemudian sklerosis dan fiksasi mukosa pada lapisan otot.Foto koagulasi infra merah, Elektrokoagulasi,Diatermi bipolar:Prinsip dari cara-cara ini hampir sama yaitu nekrosis lokal karena panas,terjadi nekrosis, fibrosis/sklerosis dan fiksasi mukosa pada jaringan otot dibawahnya.Terapi bedah. Terapi bedah dapat dilakukan dengan beberapa cara misalnya Whitehead,Milligan-Morgan atau Parks(4,5).Pemilihan modalitas terapiHemorroid derajat 1: Terapi medikBila kurang baik diganti dengan cara minimal invasiveHemorroid derajat 2:Terapi dengan cara minimal invasiveBila pasen tidak mau dapat dicoba terapi medikBila gagal dengan minimal invasive ganti dengan operasiHemorriod derajat 3:Terapi dengan minimal invasive atau operasiHemorroid derajat 4

:OperasiKesimpulanPenyakit hemorroid wlaupun bukan penyakit yang fatal,tetapi cukup mengganggu kehidupan,patogenesis penyakitini masih belum sepenuhnya difahami,tetapi faktor kongesti,hipertoni sfinkter ani dan kelemahan penyangga pleksus hemorroidalis memegang peran utama.Berbagai macam modalitas terapi.Mana yang akan dipilih hendaknya dipertimbangkan berdasarkan besar dan derajat hemorroid dan juga tentunya bergantung fasilitas serta pengalaman dari dokternya.Daftar pustaka1.Schrock TR.Examination of anorectum and disases anorectum dalam Gastrointestinal disease.Pathophysiology/diagnosis/management. edisi 5.Sleisenger MH,Fordtrand JS(ed.).WB Sauders Co.Philadelphia.1993:1499-15022.Schuster MM,Ratych RE. Anorectal diseasesdalam Bockus Gastroenterologyedisi 5.HaubrichW,Schaffner F, Berk JE(ed.).WB Saunders Co.Philadelphia.1995:1773-17763.Barnet JL.Anorectal diseasesdalam Textbook of Gastroenterology ed.3.Yamada T(ed) Lippincot William&Wilkins.Philadelphia.1999:2083-2088.

4.Keighley MRB,William NS.Surgery of the anus rectum and colon.WB Saunders Co. London.1993:295-363.5.Arullani A and Capello G.Diagnosis and Current treatment of hemorrhoidal disease. Angiology. 1994;45:560-5656.Cospite M.Double blind,Placebo-Controlled Evaluation of Clinical activity and Safety of daflon 500mg in the treatment of acute hemorrhoid.Angiology.1994;45:566-573.7.Godeberge Ph.Daflon 500 mg in the treatment of hemorrhoidal disease.A demonstrated efficacy in comparison withplacebo.Angiology.1994;45:574-578.8.Buckshee K,Takkar D,AggarwalN.Micronized flavonoid therapy in internal hemorrhoid of pregnancy.Int.J.Gyn &Obst.1997;57:145-151.

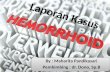
HEMORRHOID
http://blog.umy.ac.id/arsasih/hemorrhoid/
Ada banyak penyakit di daerah anus, diantaranya hemorrhoid. Hemorrhoid ini nama kerennya wasir atau ambeien. Keluhan penyakit ini antara lain: buang air besar sakit dan sulit, dubur terasa panas, adanya benjolan di dubur, serta perdarahan melalui dubur.
Hemorrhoid terjadi akibat adanya kongesti atau penumpukan vena yang disebabkan oleh gangguan aliran balik dari vena hemorrhoidalis. Faktor penyebabnya antara lain yaitu: konstipasi, diare, sering mengejan, kongesti pelvis pada kehamilan, pembesaran prostat, fibroid uteri, dan tumor rectum. Penyakit hati kronis yang disertai hipertensi portal sering mengakibatkan hemorrhoid, karena vena hemorrhoidalis superior mengalirkan darah ke dalam system portal. Selain itu, system portal tidak mempunyai katup, sehingga mudah terjadi aliran balik.
Hemorrhoid ini dibagi 2, yaitu hemorrhoid externa dan hemorrhoid interna.a. Hemorrhoid Externa. Merupakan varises vena hemorroidalis inferior. Timbul di sebelah luar otot sfingter ani, dibawah linea dentata, tertutup oleh anoderm dan berasal dari plexus hemorrhoidalis inferior. Oia, anoderm adalah jenis kulit di anus. Kulit di anus itu berbeda dgn kulit di pantat, disebutnya anoderm. Tidak ada appendices, kelenjar keringat, dan rambut.b. Hemorrhoid Interna. Merupakan varises vena hemorroidalis superior dan media. Timbul di sebelah atas atau di sebelah proximal sfingter, tertutup oleh mucosa, dan berasal dari plexus hemorrhoidalis superior. Bisa soliter (1-3 nodul) atau circuler (melingkar), letaknya sering pada tiga posisi utama yaitu jam 3,7,11.
Letak Hemorroid
Qo ada jamnya?? Iya, jadi pada pemeriksaan anus, untuk mengidentifikasi letak hemorrhoid digunakan jam. Pada pasien terlentang, arah ke atas adalah jam 12, yang ke bawah jam 6, terus jam 3 itu di kirinya pasien kanannya dokter, kalo jam 9 itu di kanannya pasien dikirinya

dokter. Jadi jam 3 di sebelah kiri pasien, jam 7 dan 11 di sebelah kanan pasien. Bingung gak? Hehe… Liat gambar monggo…
Arah jam pada pemeriksaan anus
Tidak ada klasifikasi atau derajat khusus untuk hemorrhoid externa, tapi pada hemorrhoid interna, ada 4 derajad yaitu :
1. Derajat 1 : Benjolan tidak keluar dari anus. Gimana kita bisa tahu disana ada benjolan? Jadi missal ada perdarahan saat BAB, lalu dilakukan pemeriksaan endoskopi dan hasilnya hemorrhoid, bisa dikatakan itu hemorrhoid derajat 1. Karena benjolannya belum keluar.
2. Derajat 2 : benjolan keluar waktu BAB dan masuk sendiri setelah berak.3. Derajat 3 : benjolan keluar waktu BAB, dan untuk memasukkannya lagi harus
didorong dengan jari. Kalo gak didorong, gak mau masuk. >,<4. Derajat 4 : benjolan keluar saat BAB, dan tidak dapat dimasukkan lagi. >,<”
Gejala Klinis
1. Perdarahan, menetes atau mengucur waktu mengejan , warna merah segar. Jadi kalo ada pasien yang mengeluh BAB nya berdarah tapi darahnya bercampur dengan BAB nya, maka hati-hati, itu bukan dari hemorrhoid. Bisa dari divertikula, carcinoma, atau fissure ani, atau kelainan lain.
2. Nyeri, terutama pada hemorrhoid externa. Pada hemorrhoid interna tidak nyeri kecuali ada komplikasi infeksi atau inkarserasi (retensi atau pengekangan tidak alamiah dari suatu bagian, seperti pada hernia, terjepit diluar sehingga tidak masuk lagi. – Dorland).
3. Benjolan, terlihat dari luar pada hemorrhoid externa, dan hemorrhoid interna yang prolaps (derajad IV), pada rectal toucher teraba lunak, kecuali bila ada trombus terasa keras.
Komplikasi
1. Perdarahan, akut atau kronis. Pada perdarahan akut, bisa sampai terjadi syok hipovolemik karena saking banyaknya darah yang keluar. Pada perdarahan kronis,

darah keluar sedikit demi sedikit tetapi sering sehingga dapat mempengaruhi Hb. Pernah ada pasien yang sampai kadar Hb nya 3! Itu gara-gara perdarahan kronis dari hemorrhoid.
2. Inkarserasi, infeksi dan sepsis. Jika terjadi inkarserasi kemudian infeksi, dapat terjadi sepsis.
Terapi
Operatif
- Metode Langenbeck (pada yang seoliter). Ini operasi buat yang benjolannya cuma satu.
- Modifikasi Miligan Morgan (pada yang 3 posisi (jam 3,7,11).
- Metode whiteheat (pada benjolan yang sirkuler).
Non Operatif :
- Medikamentosa. Biasanya dengan ambeven, tapi tidak terlalu bermanfaat. Kemudian ada lagi namanaya Ardium. Obat diteliti di Bandung, hasilnya nodul-nodul hemorrhoidnya mengecil saat masih diminum, tapi ketika berhenti nodulnya membesar lagi. Lagipula harganya mahal sekali, 1 tablet sampai 15-20 ribu, sehari 3 kali, diminum brapa bulan tuh.. ?
- Skleroterapi. Caranya adalah dengan disuntik menggunakan fenol atau alcohol absolute agar benjolannya nekrosis (jaringannya mati) hingga terjadi fibrosis dan mengerut, jadi tidak membesar lagi. Tapi komplikasi infeksinya banyak sekali.
- Ligasi dengan cincin karet. Biasanya ligasi ini dilakukan oleh dokter penyakit dalam, tujuannya juga adalah setelah dilakukan ligasi, maka akan terjadi nekrosis hingga terjadi fibrosis.
- Cryosurgery. Terapi ini adalah terapi dengan dibakar dingin dengan menggunakan CO2
khusus. Maksudnya juga agar terjadi nekrosis, nanti jadi fibrosis.
- Infra red cauter. Ini juga sama, agar hemorrhoidnya nekrosis hingga jadi fibrosis.
Dari semua terapi itu, saya lebih menyarankan gaya hidup sehat. Banyak makan buah dan sayur, banyak minum air, atau kalau perlu minum suplemen serat sebelum terjadi hemorrhoid. Kandungan serat dapat membantu lancar buang air besar. Selain itu, usahakan jangan mengejan, kalo belum terlalu ingin BAB, jangan dipaksa. Yang penting serat dari buah dan sayur, agar BAB lancar dan feses lunak, tidak terlalu banyak mengajan dan juga tidak keras sehingga tidak melukai anus.

Hemorrhoid adalah suatu jaringan di daerah anus yang terdiri dari pembuluh darah. Anus merupakan suatu saluran memiliki panjang kurang lebih 4 cm tempat terakhir sisa pencernaan sebelum dikeluarkan tubuh. Hemorrhoid ada pada setiap individu dan merupakan sesuatu yang normal. Pendapat di masyarakat yang menyatakan bahwa hemorrhoid merupakan suatu penyakit adalah suatu pendapat yang kurang benar. Hemorrhoid menjadi suatu penyakit bila terjadi pembengkakan dan terjadi kurang lebih 4% dari total populasi. Pembengkakan hemorrhoid dapat terjadi pada pria dan wanita di usia di atas 45 tahun.
Pembengkakan hemorrhoid dapat mengakibatkan perdarahan sehingga gejala utama yang penderita keluhkan adalah buang air besar berdarah yang terkadang disertai dengan keluarnya benjolan dari anus saat proses defekasi. Perdarahan masif dapat terjadi pada beberapa kasus karena secara anatomi, hemorrhoid terdiri dari kumpulan pembuluh darah arteri dari rectum selain pembuluh darah balik vena. Hal ini juga yang mengakibatkan darah yang keluar berwarna merah terang.
Hemorrhoid yang berasal dari bagian atas atau bagian rectum dinamakan hemorrhoid interna. Hemorrhoid yang berasal dari bagian bawah saluran anus dinamakan hemorrhoid eksternal. Secara klinis, dokter menentukan apakah hemorrhoid interna atau hemorrhoid eksterna dari lokasi hemorrhoid tersebut dari dentate line (pectinate line)
Saat ini belum ditemukan apakah penyebab pasti terjadinya pembengkakan hemorrhoid, namun keadaan ini berhubungan dengan rendahnya konsumsi serat, defekasi yang terlalu lama, dan konstipasi. Keadaan hamil juga berhubungan dengan terjadinya pembengkakan hemorrhoid selain adanya tumor di rongga panggul.
Hemorrhoid memiliki 4 stadium, yaitu:

Stadium 1 : perdarahan tanpa prolaps hemorrhoid Stadium 2 : perdarahan atau tanpa perdarhaan disertai prolaps hemorrhoid yang dapat
kembali normal Stadium 3 : prolaps hemorrhoid dan harus dibantu oleh jari agar masuk kembali ke
saluran anus Stadium 4 : prolaps hemorrhoid dan tidak dapat masuk kembali ke dalam saluran
anus. Pada stadium ini terjadi pula trombosis pada hemorrhoid.
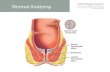
BAB2TINJAUAN PUSTAKA 2.1.Definisi Hemoroid Plexushemoroid merupakan pembuluh darah normal yang terletak pada mukosa rektum bagian distal dan anoderm. Gangguan pada hemoroid terjadi ketika plexus vaskularini membesar. Sehingga kita dapatkan pengertiannya dari “hemoroid adalah dilatasi varikosus venadari plexus hemorrhoidal inferiordan superior” (Dorland, 2002).Hemoroid adalah kumpulan dari pelebaran satu segmen atau lebih vena hemoroidalis di daerah anorektal. Hemoroid bukan sekedar pelebaran vena hemoroidalis, tetapi bersifat lebih kompleks yakni melibatkan beberapa unsur berupa pembuluh darah, jaringan lunak dan otot di sekitar anorektal (Felix, 2006). 2.2.Etiologi Hemoroid Menurut Villalba dan Abbas (2007), etiologi hemoroid sampai saat ini belum diketahui secara pasti, beberapa faktor pendukung yang terlibat diantaranya adalah: a.

Penuaan b.Kehamilan c.Hereditas d.Konstipasi atau diare kronik e.Penggunaan toilet yang berlama-lama f.Posisi tubuh, misal duduk dalam waktu yang lama g.Obesitas. Faktor-faktor tersebut berkaitan dengan kongesti vaskular dan prolapsus mukosa (Schubert dkk, 2009). Selain itu dikatakan ada hubungan antara hemoroid dengan penyakit hati maupun konsumsi alkohol (Mc Kesson Health Solution LCC, 2004)
Anatomi Anal CanalAnal canaladalah akhir dari usus besar dengan panjang 4 cm dari rektum hingga orifisium anal. Setengah bagian ke bawah dari anal canaldilapisi oleh epitel skuamosa dan setengah bagian ke atas oleh epitel kolumnar. Pada bagian yang dilapisi oleh epitel kolumnar tersebut membentuk lajur mukosa (lajur morgagni). Suplai darah bagian atas anal canalberasal dari pembuluh rektal superior sedangkan bagian bawahnya berasal dari pembuluh rektal inferior. Kedua pembuluh tersebut merupakan percabangan pembuluh darah rektal yang berasal dari arteri pudendal interna. Arteri ini adalah salah satu cabang arteri iliaka interna. Arteri-arteri tersebut akan membentuk pleksus disekitar orifisium anal. Gambar 2.1. Anatomi anal canalyang memperlihatkan pleksus hemoroid internal dan eksternal ( Penninger dan Zainea, 2001). Hemoroid adalah bantalan vaskular yang terdapat di anal canalyang biasanya ditemukan di tiga daerah utama yaitu kiri samping, kanan depan, dan bagian kanan belakang. Hemoroid berada dibawah lapisan epitel anal canaldan terdiri dari plexus arteriovenosus terutama antara cabang terminal arteri rektal

superior dan arteri hemoroid superior. Selain itu hemoroid juga menghubungkan antara arteri hemoroid dengan jaringan sekitar. Persarafan pada bagian atas anal canaldisuplai oleh plexus otonom, bagian bawah dipersarafi oleh saraf somatik rektal inferior yang merupakan akhir percabangan saraf pudendal (Snell, 2006). 2.4.Patogenesis Hemoroid Anal canal memiliki lumen triradiate yang dilapisi bantalan (cushion) atau alas dari jaringan mukosa. Bantalan ini tergantung di anal canal oleh jaringan ikat yang berasal dari sfingter anal internal dan otot longitudinal. Di dalam tiap bantalan terdapat plexus vena yang diperdarahi oleh arteriovenosus. Struktur vaskular tersebut membuat tiap bantalan membesar untuk mencegah terjadinya inkontinensia (Nisar dan Scholefield, 2003). Efek degenerasi akibat penuaan dapat memperlemah jaringan penyokong dan bersamaan dengan usaha pengeluaran feses yang keras secara berulang serta mengedan akan meningkatkan tekanan terhadap bantalan tersebut yang akan mengakibatkan prolapsus. Bantalan yang mengalami prolapsus akan terganggu aliran balik venanya. Bantalan menjadi semakin membesar dikarenakan mengedan, konsumsi serat yang tidak adekuat, berlama-lama ketika buang air besar, serta kondisi seperti kehamilan yang meningkatkan tekanan intra abdominal. Perdarahan yang timbul dari pembesaran hemoroid disebabkan oleh trauma mukosa lokal atau inflamasi yang merusak pembuluh darah di bawahnya (Acheson dan Schofield, 2006). Taweevisit dkk (2008) menyimpulkan bahwa sel mast memiliki peran multidimensional terhadap patogenesis hemoroid, melalui mediator dan sitokin yang dikeluarkan oleh granul sel mast. Pada tahap awal vasokonstriksi terjadi bersamaan dengan peningkatan vasopermeabilitas dan kontraksi otot polos yang diinduksi oleh histamin dan leukotrin. Ketika vena submukosal meregang akibat dinding pembuluh darah pada hemoroid melemah, akan terjadi ekstravasasi sel darah merah dan perdarahan. Sel mast juga melepaskan platelet-activating factorsehingga terjadi agregasi dan trombosis yang merupakan komplikasi akut hemoroid. Pada tahap selanjutnya hemoroid yang mengalami trombosis akan mengalami rekanalisasi dan resolusi. Proses ini dipengaruhi oleh kandungan granul sel mast. Termasuk diantaranya tryptase dan

chymaseuntuk degradasi jaringan stroma, heparin untuk migrasi sel endotel dan sitokin sebagai TNF-αserta interleukin 4 untuk pertumbuhan fibroblas dan proliferasi. Selanjutnya pembentukan jaringan parut akan dibantu oleh basic fibroblast growth factordari sel mast.2.5.Klasifikasi Hemoroid Hemoroid diklasifikasikan berdasarkan asalnya, dimana dentate linemenjadi batas histologis. Klasifikasi hemoroid yaitu: a.Hemoroid eksternal, berasal dari dari bagian distal dentate linedan dilapisi oleh epitel skuamos yang telah termodifikasi serta banyak persarafan serabut saraf nyeri somatik b.Hemoroid internal, berasal dari bagian proksimal dentate linedan dilapisi mukosa. c.Hemoroid internal-eksternal dilapisi oleh mukosa di bagian superior dan kulit pada bagian inferior serta memiliki serabut saraf nyeri (Corman, 2004) 2.6.Derajat Hemoroid Internal Menurut Person (2007), hemoroid internal diklasifikasikan menjadi beberapa tingkatan yakni: a.Derajat I, hemoroid mencapai lumen anal canal.b.Derajat II, hemoroid mencapai sfingter eksternal dan tampak pada saat pemeriksaan tetapi dapat masuk kembali secara spontan. c.Derajat III, hemoroid telah keluar dari anal canaldan hanya dapat masuk

kembali secara manual oleh pasienDerajat IV, hemoroid selalu keluar dan tidak dapat masuk ke anal canalmeski dimasukkan secara manual. 2.7.Gejala klinis Hemoroid Gejala klinis hemoroid dapat dibagi berdasarkan jenis hemoroid (Villalba dan Abbas, 2007) yaitu: a.Hemoroid internal 1.Prolaps dan keluarnya mukus. 2.Perdarahan. 3.Rasa tak nyaman. 4.Gatal. b.Hemoroid eksternal 1.Rasa terbakar.2.Nyeri ( jika mengalami trombosis).3.Gatal.2.8.Diagnosis Hemoroid Diagnosis hemoroid dapat dilakukan dengan melakukan: a.Anamnesis. b.Pemeriksaan fisik. c.Pemeriksaan penunjang. 2.8.1Anamnesis Hemoroid Pada anamnesis biasanya didapati bahwa pasien menemukan adanya darah segar pada saat buang air besar. Selain itu pasien juga akan mengeluhkan adanya gatal-gatal pada daerah anus. Pada derajat II hemoroid internal pasien akan merasakan adanya masa pada anus dan hal ini membuatnya tak nyaman. Pasien akan mengeluhkan nyeri pada hemoroid derajat IV yang telah mengalami trombosis (Canan, 2002)Perdarahan yang disertai dengan nyeri dapat mengindikasikan adanya trombosis hemoroid eksternal, dengan ulserasi thrombus

pada kulit. Hemoroid internal biasanya timbul gejala hanya ketika mengalami prolapsus sehingga terjadi ulserasi, perdarahan, atau trombosis. Hemoroid eksternal bisa jadi tanpa gejala atau dapat ditandai dengan rasa tak nyaman, nyeri akut, atau perdarahan akibat ulserasi dan trombosis ( Wexner, Person, dan Kaidar-person, 2006) 2.8.2Pemeriksaan Fisik HemoroidPada pemeriksaan fisik dapat ditemukan adanya pembengkakan vena yang mengindikasikan hemoroid eksternal atau hemoroid internal yang mengalami prolaps. Hemoroid internal derajat I dan II biasanya tidak dapat terlihat dari luar dan cukup sulit membedakannya dengan lipatan mukosa melalui pemeriksaan rektal kecuali hemoroid tersebut telah mengalami trombosis (Canan, 2002). Daerah perianal juga diinspeksi untuk melihat ada atau tidaknya fisura, fistula, polip, atau tumor. Selain itu ukuran, perdarahan, dan tingkat keparahan inflamasi juga harus dinilai (Nisar dan Scholefield, 2003)Pemeriksaan Penunjang Hemoroid Anal canaldan rektum diperiksa dengan menggunakan anoskopi dan sigmoidoskopi. Anoskopi dilakukan untuk menilai mukosa rektal dan mengevaluasi tingkat pembesaran hemoroid (Halverson, 2007). Side-viewingpada anoskopi merupakan instrumen yang optimal dan tepat untuk mengevaluasi hemoroid. Allonso-Coello dan Castillejo (2003) dalam Kaidar-Person, Person, dan Wexner (2007) menyatakan bahwa ketika dibandingkan dengan sigmodoskopi fleksibel, anoskopi mendeteksi dengan presentasi lebih tinggi terhadap lesi di daerah anorektal.Gejala hemoroid biasanya bersamaan dengan inflamasi pada anal canaldengan derajat berbeda. Dengan menggunakan sigmoidoskopi, anus dan rektum dapat dievaluasi untuk kondisi lain sebagai diagnosa banding untuk perdarahan rektal dan rasa tak nyaman seperti pada fisura anal dan fistula, kolitis, polip rektal, dan kanker. Pemeriksaan dengan menggunakan barium enema X-ray atau kolonoskopi harus dilakukan pada pasien dengan umur di atas 50 tahun dan pada pasien dengan perdarahan menetap setelah dilakukan pengobatan terhadap hemoroid (Canan, 2002). 2.9.Diagnosa Banding hemoroid Menurut Kaidar-Person dkk (2007) selama evaluasi awal pasien, kemungkinan penyebab lain dari gejala-gejala seperti perdarahan rektal, gatal

pada anus, rasa tak nyaman, massa serta nyeri dapat disingkirkan. Kanker kolorektal dan anal, dan melanoma anorektalmerupakan contoh penyebab gejala tersebut. Dibawah ini adalah diagnosa banding untuk gejala-gejala diatas:a.Nyeri 1.Fisura anal 2.Herpes anal 3.Proktitis ulseratif 4.Proctalgia fugaxb.Massa
Karsinoma anal 2.Perianal warts3.Skin tagsc.Nyeri dan massa 1.Hematom perianal 2.Abses 3.Pilonidal sinusd.Nyeri dan perdarahan 1.Fisura anal 2.proktitis e.Nyeri, massa, dan perdarahan Hematom perianal ulseratif f.Massa dan perdarahan Karsinoma anal g.Perdarahan 1.Polips kolorektal

2.Karsinoma kolorektal 3.Karsinoma anal 2.10. Penatalaksanaan Hemoroid Menurut Acheson dan Scholefield (2006), penatalaksanaan hemoroid dapat dilakukan dengan beberapa cara sesuai dengan jenis dan derajat daripada hemoroid. Penatalaksanaan Konservatif Sebagian besar kasus hemoroid derajat I dapat ditatalaksana dengan pengobatan konservatif. Tatalaksana tersebut antara lain koreksi konstipasi jika ada, meningkatkan konsumsi serat, laksatif, dan menghindari obat-obatan yang dapat menyebabkan kostipasi seperti kodein (Daniel, 2010) Penelitian meta-analisis akhir-akhir ini membuktikan bahwa suplemen serat dapat memperbaiki gejala dan perdarahan serta dapat direkomendasikan
pada derajat awal hemoroid (Zhou dkk, 2006). Perubahan gaya hidup lainnya seperti meningkatkan konsumsi cairan, menghindari konstipasi dan mengurangi mengejan saat buang air besar dilakukan pada penatalaksanaan awal dan dapat membantu pengobatan serta pencegahan hemoroid, meski belum banyak penelitian yang mendukung hal tersebut. Kombinasi antara anestesi lokal, kortikosteroid, dan antiseptik dapat mengurangi gejala gatal-gatal dan rasa tak nyaman pada hemoroid. Penggunaan steroid yang berlama-lama harus dihindari untuk mengurangi efek samping. Selain itu suplemen flavonoid dapat membantu mengurangi tonus vena, mengurangi hiperpermeabilitas serta efek antiinflamasi meskipun belum diketahui bagaimana mekanismenya (Acheson dan Scholrfield, 2008). Pembedahan Acheson dan Scholfield (2008) menyatakan apabila hemoroid internal derajat I yang tidak membaik dengan penatalaksanaan konservatif maka dapat dilakukan tindakan pembedahan. HIST (Hemorrhoid Institute of South Texas) menetapkan indikasi tatalaksana pembedahan hemoroid antara lain: a.Hemoroid internal derajat II berulang.b.Hemoroid derajat III dan IV dengan gejala.c.Mukosa rektum menonjol keluar anus.d.Hemoroid derajat I dan II dengan penyakit penyerta seperti fisura.e.Kegagalan penatalaksanaan konservatif.f.Permintaan pasien.Pembedahan yang sering dilakukan yaitu:

1.Skleroterapi. Teknik ini dilakukan menginjeksikan 5 mL oil phenol 5 %, vegetable oil, quinine, dan urea hydrochlorate atau hypertonic salt solution. Lokasi injeksi adalah submukosa hemoroid. Efek injeksi sklerosan tersebut adalah edema, reaksi inflamasi dengan proliferasi fibroblast, dan trombosis intravaskular. Reaksi ini akan menyebabkan fibrosis pada sumukosa hemoroid. Hal ini akan mencegah atau mengurangi prolapsus jaringan hemoroid (Kaidar-Person dkk, 2007). Senapati (1988) dalam Acheson dan Scholfield (2009) menyatakan teknik ini murah dan mudah dilakukan, tetapi jarang dilaksanakan karena tingkat kegagalan yang tinggi. 2.Rubber band ligation. Ligasi jaringan hemoroid dengan rubber bandmenyebabkan nekrosis iskemia, ulserasi dan scarringyang akan menghsilkan fiksasi jaringan ikat ke dinding rektum. Komplikasi prosedur ini adalah nyeri dan perdarahan. 3.Infrared thermocoagulation. Sinar infra merah masuk ke jaringan dan berubah menjadi panas. Manipulasi instrumen tersebut dapat digunakan untuk mengatur banyaknya jumlah kerusakan jaringan. Prosedur ini menyebabkan koagulasi, oklusi, dan sklerosis jaringan hemoroid. Teknik ini singkat dan dengan komplikasi yang minimal. 4.Bipolar Diathermy. Menggunakan energi listrik untuk mengkoagulasi jaringan hemoroid dan pembuluh darah yang memperdarahinya. Biasanya digunakan pada hemoroid internal derajat rendah. 5.Laser haemorrhoidectomy.6.Doppler ultrasound guided haemorrhoid artery ligation. Teknik ini dilakukan dengan menggunakan proktoskop yang dilengkapi dengan

doppler probeyang dapat melokalisasi arteri.Kemudian arteri yang memperdarahi jaringan hemoroid tersebut diligasi menggunakan absorbable suture. Pemotongan aliran darah ini diperkirakan akan mengurangi ukuran hemoroid. 7.Cryotherapy. Teknik ini dilakukan dengan menggunakan temperatur yang sangat rendah untuk merusak jaringan. Kerusakan ini disebabkan kristal yang terbentuk di dalam sel, menghancurkan membran sel dan jaringan. Namun prosedur ini menghabiskan banyak waktu dan hasil yang cukup mengecewakan. Cryotherapyadalah teknik yang paling jarang dilakukan untuk hemoroid (American Gastroenterological Association, 2004)Stappled Hemorrhoidopexy. Teknik dilakukan dengan mengeksisi jaringan hemoroid pada bagian proksimal dentate line. Keuntungan pada stappled hemorrhoidopexyadalah berkurangnya rasa nyeri paska operasi selain itu teknik ini juga aman dan efektif sebagai standar hemorrhoidectomy (Halverson, 2007).Menurut Nagie (2007), pencegahan hemoroid dapat dilakukan dengan: 1.Konsumsi serat 25-30 gram sehari. Makanan tinggi serat seperti buah-buahan, sayur-mayur, dan kacang-kacangan menyebabkan feses menyerap air di kolon. Hal ini membuat feses lebih lembek dan besar, sehingga mengurangi proses mengedan dan tekanan pada vena anus. 2.Minum air sebanyak 6-8 gelas sehari 3.Mengubah kebiasaan buang air besar. Segera ke kamar mandi saat merasa akan buang air besar, jangan ditahan karena akan memperkeras feses. Hindari mengedan

Anus and perianal areaGeneralAnatomy
Reviewers: Charles Ladoulis, M.D. (see Reviewers page) Revised: 13 April 2013, last major update May 2012Copyright: (c) 2002-2012, PathologyOutlines.com, Inc.
General=========================================================================Anal canal:● Tubular structure 3-4 cm long● Derived from cloaca (distal hindgut) and arises at level of prostatic apex, is directed downward and backward, and ends at anus● Boundaries are proximal and distal margins of internal sphincter muscle, and includes part of rectum● Embryologically divided by urogenital septum (cloacal membrane) into anterior GU and posterior GI compartments, and separated from perianal ectoderm by anal membrane, which ruptures at week 7 of gestation
Classic anatomic definition of anal canal:● Between proximal and distal margins of internal sphincter muscle, which includes part of rectum
Clinical AJCC definition of anal canal:● Begins at puborectalis sling at apex of anal sphincter complex (palpable as anorectal ring, but difficult for pathologists to identify)● Ends at squamous mucocutaneous junction with perianal skin; includes 1-2 cm of rectal-type glandular mucosa and possibly transitional mucosa at dentate line
Histologic definition of anal canal:● Anal transitional zone and squamous epithelium down to the perianal skin; cannot be identified by clinicians● Note: “columns”, “valves” and “sinuses” below are macroscopic landmarks, which may not correspond precisely to microscopic structures
● Anal columns of Morgagni: longitudinal folds just distal to dentate line, analogous to lower rectum’s rectal columns of Morgagni; less pronounced in adults● Anal papillae: raised toothlike projections on anal columns; extend proximally into rectum● Anal sinuses of Morgagni: depressions between anal columns● Anal crypts of Morgagni: minute pockets with anal valves as boundary; site of discharge of anal glands
Anal valves:● Also called semilunar valves or transverse plicae● Connect distal ends of anal columns● Identifiable in children, often obscured in adults
Anal cushions:● Normal structures of anal canal that contribute to anal closure by close apposition to each other● Contain blood vessels, connective tissue, smooth muscle; vessels

contain abundant smooth muscle● Resemble erectile tissue due to numerous arteriovenous communications
Anal verge:● Also called Hilton’s line or anal margin;● Junction between anal canal and anal skin● Mucosa contains cutaneous adnexae
● Corpus cavernosum recti: network formed by peculiar vessels with a complex convoluted appearance● Dentate (pectinate) line: midpoint of anal canal, formed by anal valves; circumferential musculature of canal
Musculature of anal canal
General=========================================================================● Muscularis mucosa: continues from rectum through upper anal transitional zone ● Presence of muscle fibers in lamina propria indicates mucosal prolapse syndrome● Musculus submucosae ani: fibers from intersphincteric longitudinal muscle which pass through internal sphincter and from the internal sphincter itself; form a network around the vascular plexus
Internal anal sphincter:● Continuation of circular muscle of rectum, but thicker (5-8 mm); ends 5-19 mm below dentate line
Intersphincteric longitudinal muscle:● Between internal and external sphincters● Contains fibers from longitudinal muscle layer of rectum and levator ani muscles● Distally breaks up into septa that diverge fan-wise through subcutaneous layer of external sphincter and ends in corium, which forms characteristic corrugation of perianal skin
External anal sphincter:● Consists of superficial, subcutaneous and deep parts; provides voluntary control of defecation
Regional lymph node drainage:● Above dentate line - anorectal, perirectal, paravertebral nodes● Below dentate line - superficial inguinal nodes
● Arterial supply: superior, middle and inferior rectal arteries● Venous supply: superior rectal vein

Inner wall of the lower end of the rectum and anus. On the right the mucous membrane has been removed to show the dilatation of the veins and how they pass through the muscular
wall to anastomose with the external hemorrhoidal plexus. (Luschka.)

Henry Gray (1821–1865). Anatomy of the Human Body. 1918.
2h. The Large Intestine
(Intestinum Crassum)
The large intestine extends from the end of the ileum to the anus. It is about 1.5 meters long, being one-fifth of the whole extent of the intestinal canal. Its caliber is largest at its commencement at the cecum, and gradually diminishes as far as the rectum, where there is a dilatation of considerable size just above the anal canal. It differs from the small intestine in its greater caliber, its more fixed position, its sacculated form, and in possessing certain appendages to its external coat, the appendices epiploicæ. Further, its longitudinal muscular fibers do not form a continuous layer around the gut, but are arranged in three longitudinal bands or tæniæ. The large intestine, in its course, describes an arch which surrounds the convolutions of the small intestine. It commences in the right iliac region, in a dilated part, the cecum. It ascends through the right lumbar and hypochondriac regions to the under surface of the liver; it here takes a bend, the right colic flexure, to the left and passes transversely across the abdomen on the confines of the epigastric and umbilical regions, to the left hypochondriac region; it then bends again, the left colic flexure, and descends through the left lumbar and iliac regions to the pelvis, where it forms a bend called the sigmoid flexure; from this it is continued along the posterior wall of the pelvis to the anus. The large intestine is divided into the cecum, colon, rectum, and anal canal.
1
The Cecum (intestinum cæcum) (Fig. 1073), the commencement of the large intestine, is the large blind pouch situated below the colic valve. Its blind end is directed downward, and its open end upward, communicating directly with the colon, of which this blind pouch appears to be the beginning or head, and hence the old name of caput cæcum coli was applied to it. Its size is variously estimated by different authors, but on an average it may be said to be 6.25 cm. in length and 7.5 in breadth. It is situated in the right iliac fossa, above the lateral half of the inguinal ligament: it rests on the Iliacus and Psoas major, and usually lies in contact with the anterior abdominal wall, but the greater omentum and, if the cecum be empty, some coils of small intestine may lie in front of it. As a rule, it is entirely enveloped by peritoneum, but in a certain number of cases (5 per cent., Berry) the peritoneal covering is not complete, so that the upper part of the posterior surface is uncovered and connected to the iliac fascia by connective tissue. The cecum lies quite free in the abdominal cavity and enjoys a considerable amount of movement, so that it may become herniated down the right inguinal canal, and has occasionally been found in an inguinal hernia on the left side. The cecum varies in shape, but, according to Treves, in man it may be classified under one of four types. In early fetal life it is short, conical, and broad at the base, with its apex turned upward and medialward toward the ileocolic junction. It then resembles the cecum of some monkeys, e. g., mangabey monkey. As the fetus grows the
2

cecum increases in length more than in breadth, so that it forms a longer tube than in the primitive form and without the broad base, but with the same inclination of the apex toward the ileocolic junction. This form is seen in other monkeys, e. g., the spider monkey. As development goes on, the lower part of the tube ceases to grow and the upper part becomes greatly increased, so that at birth there is a narrow tube, the vermiform process, hanging from a conical projection, the cecum. This is the infantile form, and as it persists throughout life in about 2 per cent. of cases, it is regarded by Treves as the first of his four types of human ceca. The cecum is conical and the appendix rises from its apex. The three longitudinal bands start from the appendix and are equidistant from each other. In the second type, the conical cecum has become quadrate by the growing out of a saccule on either side of the anterior longitudinal band. These saccules are of equal size, and the appendix arises from between them, instead of from the apex of a cone. This type is found in about 3 per cent. of cases. The third type is the normal type of man. Here the two saccules, which in the second type were uniform, have grown at unequal rates: the right with greater rapidity than the left. In consequence of this an apparently new apex has been formed by the growing downward of the right saccule, and the original apex, with the appendix attached, is pushed over to the left toward the ileocolic junction. The three longitudinal bands still start from the base of the vermiform process, but they are now no longer equidistant from each other, because the right saccule has grown between the anterior and posterolateral bands, pushing them over to the left. This type occurs in about 90 per cent. of cases. The fourth type is merely an exaggerated condition of the third; the right saccule is still larger, and at the same time the left saccule has become atrophied, so that the original apex of the cecum, with the vermiform process, is close to the ileocolic junction, and the anterior band courses medialward to the same situation. This type is present in about 4 per cent. of cases.
FIG. 1073– The cecum and vermiform process, with their arteries. (See enlarged image)
The Vermiform Process or Appendix (processus vermiformis) (Fig. 1073) is a long, narrow, worm-shaped tube, which starts from what was originally the apex of the cecum, and may pass in one of several directions: upward behind the cecum; to the left behind the ileum and mesentery;
3

or downward into the lesser pelvis. It varies from 2 to 20 cm. in length, its average being about 8.3 cm. It is retained in position by a fold of peritoneum (mesenteriole), derived from the left leaf of the mesentery. This fold, in the majority of cases, is more or less triangular in shape, and as a rule extends along the entire length of the tube. Between its two layers and close to its free margin lies the appendicular artery (Fig. 1073). The canal of the vermiform process is small, extends throughout the whole length of the tube, and communicates with the cecum by an orifice which is placed below and behind the ileocecal opening. It is sometimes guarded by a semilunar valve formed by a fold of mucous membrane, but this is by no means constant.
Structure.—The coats of the vermiform process are the same as those of the intestine: serous, muscular, submucous, and mucous. The serous coat forms a complete investment for the tube, except along the narrow line of attachment of its mesenteriole in its proximal two-thirds. The longitudinal muscular fibers do not form three bands as in the greater part of the large intestine, but invest the whole organ, except at one or two points where both the longitudinal and circular fibers are deficient so that the peritoneal and submucous coats are contiguous over small areas.
4
The circular muscle fibers form a much thicker layer than the longitudinal fibers, and are separated from them by a small amount of connective tissue. The submucous coat is well marked, and contains a large number of masses of lymphoid tissue which cause the mucous membrane to bulge into the lumen and so render the latter of small size and irregular shape. The mucous membrane is lined by columnar epithelium and resembles that of the rest of the large intestine, but the intestinal glands are fewer in number (Fig. 1074).
5
FIG. 1074– Transverse section of human vermiform process. X 20. (See enlarged image)
The Colic Valve (valvula coli; ileocecal valve) (Fig. 1075).—The lower end of the ileum ends by opening into the medial and back part of the large intestine, at the point of junction of the cecum with the colon. The opening is guarded by a valve, consisting of two segments or lips, which
6

project into the lumen of the large intestine. If the intestine has been inflated and dried, the lips are of a semilunar shape. The upper one, nearly horizontal in direction, is attached by its convex border to the line of junction of the ileum with the colon; the lower lip, which is longer and more concave, is attached to the line of junction of the ileum with the cecum. At the ends of the aperture the two segments of the valve coalesce, and are continued as narrow membranous ridges around the canal for a short distance, forming the frenula of the valve. The left or anterior end of the aperture is rounded; the right or posterior is narrow and pointed. In the fresh condition, or in specimens which have been hardened in situ, the lips project as thick cushion-like folds into the lumen of the large gut, while the opening between them may present the appearance of a slit or may be somewhat oval in shape.
Each lip of the valve is formed by a reduplication of the mucous membrane and of the circular muscular fibers of the intestine, the longitudinal fibers and peritoneum being continued uninterruptedly from the small to the large intestine.
7
The surfaces of the valve directed toward the ileum are covered with villi, and present the characteristic structure of the mucous membrane of the small intestine; while those turned toward the large intestine are destitute of villi, and marked with the orifices of the numerous tubular glands peculiar to the mucous membrane of the large intestine. These differences in structure continue as far as the free margins of the valve. It is generally maintained that this valve prevents reflux from the cecum into the ileum, but in all probability it acts as a sphincter around the end of the ileum and prevents the contents of the ileum from passing too quickly into the cecum.
8
The Colon is divided into four parts: the ascending, transverse, descending, and sigmoid. 9
FIG. 1075– Interior of the cecum and lower end of ascending colon, showing colic valve. (See enlarged image)
The Ascending Colon (colon ascendens) is smaller in caliber than the cecum, with which it is continuous. It passes upward, from its commencement at the cecum, opposite the colic valve, to the under surface of the right lobe of the liver, on the right of the gall-bladder, where it is lodged

in a shallow depression, the colic impression; here it bends abruptly forward and to the left, forming the right colic (hepatic) flexure (Fig. 1056). It is retained in contact with the posterior wall of the abdomen by the peritoneum, which covers its anterior surface and sides, its posterior surface being connected by loose areolar tissue with the Iliacus, Quadratus lumborum, aponeurotic origin of Transversus abdominis, and with the front of the lower and lateral part of the right kidney. Sometimes the peritoneum completely invests it, and forms a distinct but narrow mesocolon. 169 It is in relation, in front, with the convolutions of the ileum and the abdominal parietes.
The Transverse Colon (colon transversum) the longest and most movable part of the colon, passes with a downward convexity from the right hypochondriac region across the abdomen, opposite the confines of the epigastric and umbilical zones, into the left hypochondriac region, where it curves sharply on itself beneath the lower end of the spleen, forming the left colic (splenic) flexure. In its course it describes an arch, the concavity of which is directed backward and a little upward; toward its splenic end there is often an abrupt U-shaped curve which may descend lower than the main curve. It is almost completely invested by peritoneum, and is connected to the inferior border of the pancreas by a large and wide duplicature of that membrane, the transverse mesocolon. It is in relation, by its upper surface, with the liver and gall-bladder, the greater curvature of the stomach, and the lower end of the spleen; by its under surface, with the small intestine; by its anterior surface, with the anterior layers of the greater omentum and the abdominal parietes; its posterior surface is in relation from right to left with the descending portion of the duodenum, the head of the pancreas, and some of the convolutions of the jejunum and ileum.
11
The left colic or splenic flexure (Fig. 1056) is situated at the junction of the transverse and descending parts of the colon, and is in relation with the lower end of the spleen and the tail of the pancreas; the flexure is so acute that the end of the transverse colon usually lies in contact with the front of the descending colon. It lies at a higher level than, and on a plane posterior to, the right colic flexure, and is attached to the diaphragm, opposite the tenth and eleventh ribs, by a peritoneal fold, named the phrenicocolic ligament, which assists in supporting the lower end of the spleen (see page 1158).
12

FIG. 1076– Iliac colon, sigmoid or pelvic colon, and rectum seen from the front, after removal of pubic bones and bladder. (See enlarged image)
The Descending Colon 170 (colon descendens) passes downward through the left hypochondriac and lumbar regions along the lateral border of the left kidney. At the lower end of the kidney it turns medialward toward the lateral border of the Psoas, and then descends, in the angle between Psoas and Quadratus lumborum, to the crest of the ilium, where it ends in the iliac colon. The peritoneum covers its anterior surface and sides, while its posterior surface is connected by areolar tissue with the lower and lateral part of the left kidney, the aponeurotic origin of the Transversus abdominis, and the Quadratus lumborum (Fig. 1056). It is smaller in caliber and more deeply placed than the ascending colon, and is more frequently covered with peritoneum on its posterior surface than the ascending colon (Treves). In front of it are some coils of small intestine.
13
The Iliac Colon (Fig. 1076) is situated in the left iliac fossa, and is about 12 to 15 cm. long. It begins at the level of the iliac crest, where it is continuous with the descending colon, and ends in the sigmoid colon at the superior aperture of the lesser pelvis. It curves downward and medialward in front of the Iliacus and Psoas, and, as a rule, is covered by peritoneum on its sides and anterior surface only.
14

FIG. 1077– The posterior aspect of the rectum exposed by removing the lower part of the sacrum and the coccyx. (See enlarged image)
The Sigmoid Colon (colon sigmoideum; pelvic colon; sigmoid flexure) (Fig. 1076) forms a loop which averages about 40 cm. in length, and normally lies within the pelvis, but on account of its freedom of movement it is liable to be displaced into the abdominal cavity. It begins at the superior aperture of the lesser pelvis, where it is continuous with the iliac colon, and passes transversely across the front of the sacrum to the right side of the pelvis; it then curves on itself and turns toward the left to reach the middle line at the level of the third piece of the sacrum, where it bends downward and ends in the rectum. It is completely surrounded by peritoneum, which forms a mesentery (sigmoid mesocolon), which diminishes in length from the center toward the ends of the loop, where it disappears, so that the loop is fixed at its junctions with the iliac colon and rectum, but enjoys a considerable range of movement in its central portion. Behind the sigmoid colon are the external iliac vessels, the left Piriformis, and left sacral plexus of nerves; in front, it is separated from the bladder in the male, and the uterus in the female, by some coils of the small intestine.
15
The Rectum (intestinum rectum) (Fig. 1077) is continuous above with the sigmoid colon, while below it ends in the anal canal. From its origin at the level of the third sacral vertebra it passes downward, lying in the sacrococcygeal curve, and extends for about 2.5 cm. in front of, and a little below, the tip of the coccyx, as far as the apex of the prostate. It then bends sharply backward into the anal canal. It therefore presents two antero-posterior curves: an upper, with its convexity backward, and a lower, with its convexity forward. Two lateral curves are also described, one to the right opposite the junction of the third and fourth sacral vertebræ, and the other to the left, opposite the left sacrococcygeal articulation; they are, however, of little importance. The rectum is about 12 cm. long, and at its commencement its caliber is similar to that of the sigmoid colon, but near its termination it is dilated to form the rectal ampulla. The
16

rectum has no sacculations comparable to those of the colon, but when the lower part of the rectum is contracted, its mucous membrane is thrown into a number of folds, which are longitudinal in direction and are effaced by the distension of the gut. Besides these there are certain permanent transverse folds, of a semilunar shape, known as Houston’s valves (Fig. 1078). They are usually three in number; sometimes a fourth is found, and occasionally only two are present. One is situated near the commencement of the rectum, on the right side; a second extends inward from the left side of the tube, opposite the middle of the sacrum; a third, the largest and most constant, projects backward from the forepart of the rectum, opposite the fundus of the urinary bladder. When a fourth is present, it is situated nearly 2.5 cm. above the anus on the left and posterior wall of the tube. These folds are about 12 mm. in width, and contain some of the circular fibers of the gut. In the empty state of the intestine they overlap each other, as Houston remarks, so effectually as to require considerable maneuvering to conduct a bougie or the finger along the canal. Their use seems to be, “to support the weight of fecal matter, and prevent its urging toward the anus, where its presence always excites a sensation demanding its discharge. 171
The peritoneum is related to the upper two-thirds of the rectum, covering at first its front and sides, but lower down its front only; from the latter it is reflected on to the seminal vesicles in the male and the posterior vaginal wall in the female.
17
FIG. 1078– Coronal section of rectum and anal canal. (See enlarged image)
The level at which the peritoneum leaves the anterior wall of the rectum to be reflected on to the viscus in front of it is of considerable importance from a surgical point of view, in connection with the removal of the lower part of the rectum. It is higher in the male than in the female. In the former the height of the rectovesical excavation is about 7.5 cm., i. e., the height to which an ordinary index finger can reach from the anus. In the female the height of the rectouterine excavation is about 5.5 cm. from the anal orifice. The rectum is surrounded by a dense tube of
18

fascia derived from the fascia endopelvina, but fused behind with the fascia covering the sacrum and coccyx. The facial tube is loosely attached to the rectal wall by areolar tissue in order to allow of distension of the viscus.
Relations of the Rectum.—The upper part of the rectum is in relation, behind, with the superior hemorrhoidal vessels, the left Piriformis, and left sacral plexus of nerves, which separate it from the pelvic surfaces of the sacral vertebræ; in its lower part it lies directly on the sacrum, coccyx, and Levatores ani, a dense fascia alone intervening; in front, it is separated above, in the male, from the fundus of the bladder; in the female, from the intestinal surface of the uterus and its appendages, by some convolutions of the small intestine, and frequently by the sigmoid colon; below, it is in relation in the male with the triangular portion of the fundus of the bladder, the vesiculæ seminales, and ductus deferentes, and more anteriorly with the posterior surface of the prostate; in the female, with the posterior wall of the vagina.
19
FIG. 1079– Coronal section through the anal canal. (Symington.) B. Cavity of urinary bladder. V.D. Ductus deferens. S.V. Seminal vesicle. R. Second part of rectum. A.C. Anal canal. L.A. Levator ani.
I.S. Sphincter ani internus. E.S. Sphinear ani externus. (See enlarged image)

FIG. 1080– The interior of the anal cami and lower part of the rectum, showing the columns of Morgagni and the anal valves between their lower ends. The columns were more numerous in
the specimen than usual. (Cunningham.) (See enlarged image)
The Anal Canal (pars analis recti) (Figs. 1079, 1080, 1081), or terminal portion of the large intestine, begins at the level of the apex of the prostate, is directed downward and backward, and ends at the anus. It forms an angle with the lower part of the rectum, and measures from 2.5 to 4 cm. in length. It has no peritoneal covering, but is invested by the Sphincter ani internus, supported by the Levatores ani, and surrounded at its termination by the Sphincter ani externus. In the empty condition it presents the appearance of an antero-posterior longitudinal slit. Behind it is a mass of muscular and fibrous tissue, the anococcygeal body (Symington); in front of it, in the male, but separated by connective tissue from it, are the membranous portion and bulb of the urethra, and the fascia of the urogenital diaphragm; and in the female it is separated from the lower end of the vagina by a mass of muscular and fibrous tissue, named the perineal body.
20
FIG. 1081– Inner wall of the lower end of the rectum and anus. On the right the mucous membrane has been removed to show the dilatation of the veins and how they pass through the
muscular wall to anastomose with the external hemorrhoidal plexus. (Luschka.) (See enlarged image)
The lumen of the anal canal presents, in its upper half, a number of vertical folds, produced by 21

an infolding of the mucous membrane and some of the muscular tissue. They are known as the rectal columns [Morgagni] (Fig. 1078), and are separated from one another by furrows (rectal sinuses), which end below in small valve-like folds, termed anal valves, which join together the lower ends of the rectal columns.
FIG. 1082– Section of mucous membrane of human rectum. (Sobotta.) X 60. (See enlarged image)
Structure of the Colon.—The large intestine has four coats: serous, muscular, areolar, and mucous.
22
The serous coat (tunica serosa) is derived from the peritoneum, and invests the different portions of the large intestine to a variable extent. The cecum is completely covered by the serous membrane, except in about 5 per cent. of cases where the upper part of the posterior surface is uncovered. The ascending, descending, and iliac parts of the colon are usually covered only in front and at the sides; a variable amount of the posterior surface is uncovered. 172 The transverse colon is almost completely invested, the parts corresponding to the attachment of the greater omentum and transverse mesocolon being alone excepted. The sigmoid colon is entirely surrounded. The rectum is covered above on its anterior surface and sides; below, on its anterior aspect only; the anal canal is entirely devoid of any serous covering. In the course of the colon the peritoneal coat is thrown into a number of small pouches filled with fat, called appendices epiploicæ. They are most numerous on the transverse colon.
23
The muscular coat (tunica muscularis) consists of an external longitudinal, and an internal circular, layer of non-striped muscular fibers:
24
The longitudinal fibers do not form a continuous layer over the whole surface of the large intestine. In the cecum and colon they are especially collected into three flat longitudinal bands (tænæi coli), each of about 12 mm. in width; one, the posterior, is placed along the attached border of the intestine; the anterior, the largest, corresponds along the arch of the colon to the attachment of the greater omentum, but is in front in the ascending, descending, and iliac parts
25

of the colon, and in the sigmoid colon; the third, or lateral band, is found on the medial side of the ascending and descending parts of the colon, and on the under aspect of the transverse colon. These bands are shorter than the other coats of the intestine, and serve to produce the sacculi which are characteristic of the cecum and colon; accordingly, when they are dissected off, the tube can be lengthened, and its sacculated character disappears. In the sigmoid colon the longitudinal fibers become more scattered; and around the rectum they spread out and form a layer, which completely encircles this portion of the gut, but is thicker on the anterior and posterior surfaces, where it forms two bands, than on the lateral surfaces. In addition, two bands of plain muscular tissue arise from the second and third coccygeal vertebræ, and pass downward and forward to blend with the longitudinal muscular fibers on the posterior wall of the anal canal. These are known as the Rectococcygeal muscles.
FIG. 1083– The bloodvessels of the rectum and anus, showing the distribution and anastomosis on the posterior surface near the termination of the gut. (Poirier and Charpy) (See enlarged image)
The circular fibers form a thin layer over the cecum and colon, being especially accumulated in the intervals between the sacculi; in the rectum they form a thick layer, and in the anal canal they become numerous, and constitute the Sphincter ani internus.
26
The areolar coat (tela submucosa; submucous coat) connects the muscular and mucous layers closely together.
27
The mucous membrane (tunica mucosa) in the cecum and colon, is pale, smooth, destitute of villi, and raised into numerous crescentic folds which correspond to the intervals between the sacculi. In the rectum it is thicker, of a darker color, more vascular, and connected loosely to the
28

muscular coat, as in the esophagus.
As in the small intestine, the mucous membrane (Fig. 1082) consists of a muscular layer, the muscularis mucosæ; a quantity of retiform tissue in which the vessels ramify; a basement membrane and epithelium which is of the columnar variety, and resembles the epithelium found in the small intestine. The mucous membrane of the large intestine presents for examination glands and solitary lymphatic nodules.
29
The glands of the great intestine are minute tubular prolongations of the mucous membrane arranged perpendicularly, side by side, over its entire surface; they are longer, more numerous, and placed in much closer apposition than those of the small intestine; and they open by minute rounded orifices upon the surface, giving it a cribriform appearance. Each gland is lined by short columnar epithelium and contains numerous goblet cells.
30
The solitary lymphatic nodules (noduli lymphatic solitarii) (Fig. 1082) of the large intestine are most abundant in the cecum and vermiform process, but are irregularly scattered also over the rest of the intestine. They are similar to those of the small intestine.
31
Vessels and Nerves.—The arteries supplying the colon are derived from the colic and sigmoid branches of the mesenteric arteries. They give off large branches, which ramify between and supply the muscular coats, and after dividing into small vessels in the submucous tissue, pass to the mucous membrane. The rectum is supplied by the superior hemorrhoidal branch of the inferior mesenteric, and the anal canal by the middle hemorrhoidal from the hypogastric, and the inferior hemorrhoidal from the internal pudendal artery. The superior hemorrhoidal, the continuation of the inferior mesenteric, divides into two branches, which run down either side of the rectum to within about 12.5 cm. of the anus; they here split up into about six branches which pierce the muscular coat and descend between it and the mucous membrane in a longitudinal direction, parallel with each other as far as the Sphincter ani internus, where they anastomose with the other hemorrhoidal arteries and form a series of loops around the anus. The veins of the rectum commence in a plexus of vessels which surrounds the anal canal. In the vessels forming this plexus are smaller saccular dilatations just within the margin of the anus; from the plexus about six vessels of considerable size are given off. These ascend between the muscular and mucous coats for about 12.5 cm., running parallel to each other; they then pierce the muscular coat, and, by their union, form a single trunk, the superior hemorrhoidal vein. This arrangement is termed the hemorrhoidal plexus; it communicates with the tributaries of the middle and inferior hemorrhoidal veins, at its commencement, and thus a communication is established between the systemic and portal circulations. The lymphatics of the large intestine are described on page 711. The nerves are derived from the sympathetic plexuses around the branches of the superior and inferior mesenteric arteries. They are distributed in a similar way to those found in the small intestine.
32
Congenital Hernia.—There are some varieties of oblique inguinal hernia (Fig. 1084) depending upon congenital defects in the saccus vaginalis, the pouch of peritoneum which precedes the
33

descent of the testis. Normally this pouch is closed before birth, closure commencing at two points, viz., at the abdominal inguinal ring and at the top of the epididymis, and gradually extending until the whole of the intervening portion is converted into a fibrous cord. From failure in the completion of this process, variations in the relation of the hernial protrusion to the testis and tunica vaginalis are produced; these constitute distinct varieties of inguinal hernia, viz., the hernia of the funicular process and the complete congenital variety.
FIG. 1084– Varieties of oblique inguinal hernia. (See enlarged image)
Where the saccus vaginalis remains patent throughout, the cavity of the tunica vaginalis communicates directly with that of the peritoneum. The intestine descends along this pouch into the cavity of the tunica vaginalis which constitutes the sac of the hernia, and the gut lies in contact with the testis. Though this form of hernia is termed complete congenital, the term does not imply that the hernia existed at birth, but merely that a condition is present which may allow of the descent of the hernia at any moment. As a matter of fact, congenital herniæ frequently do not appear until adult life.
34
Where the processus vaginalis is occluded at the lower point only, i.e., just above the testis, the intestine descends into the pouch of peritoneum as far as the testis, but is prevented from entering the sac of the tunica vaginalis by the septum which has formed between it and the pouch. This is known as hernia into the funicular process or incomplete congenital hernia; it differs from the former in that instead of enveloping the testis it lies above it.
35
Note 169. Treves states that, after a careful examination of one hundred subjects, he found that in fifty-two there was neither an ascending nor a descending mesocolon. In twenty-two there was a descending mesocolon, but no trace of a corresponding fold on the other side. In fourteen subjects there was a mesocolon to both the ascending and the descending segments of the bowel; while in

the remaining twelve there was an ascending mesocolon, but no corresponding fold on the left side. It follows, therefore, that in performing lumbar colotomy a mesocolon may be expected upon the left side in 36 per cent. of all cases, and on the right in 26 per cent.—The Anatomy of the Intestinal Canal and Peritoneum in Man, 1885, p. 55. [back]
Note 170. In the Basle nomenclature the descending colon is the portion between the left colic flexure and the superior aperture of the lesser pelvis; it is, however, convenient to describe its lowest part as the iliac colon. [back]
Note 171. Paterson (“The Form of the Rectum,” Journal of Anatomy and Physiology, vol. xliii) utilizes the third fold for the purpose of dividing the rectum into an upper and a lower portion; he considers the latter “to be just as much a duct as the narrower anal canal below,” and maintains that, under normal conditions, it does not contain feces except during the act of defecation. [back]
Note 172. See footnote, p. 1183. [back]
AUTHOR: Gray, Henry, 1825–1861.
TITLE: Anatomy of the human body, by Henry Gray. 20th ed., thoroughly rev. and re-edited by Warren H. Lewis.
PUBLISHED: Philadelphia: Lea & Febiger, 1918.
PHYSICAL DETAILS:
1396 p.: ill. (some col.); 27 cm. Includes bibliographies and index.
OTHER AUTHOR:
Lewis, Warren Harmon, 1870–.
ISBN: 1-58734-102-6.
CITATION: Gray, Henry. Anatomy of the Human Body. Philadelphia: Lea & Febiger, 1918; Bartleby.com, 2000. www.bartleby.com/107/. [Date of Printout].
ON-LINE ED.: Published May 2000 by Bartleby.com; © 2000 Copyright Bartleby.com, Inc. (Terms of Use).
http://www.bartleby.com/br/107.html
BAHAN DARI MEDSCAPE (ANATOMI ANAL CANAL)

http://emedicine.medscape.com/article/1990236-overview#a30The anal canal is the most terminal part of the lower GI tract/large intestine, which lies between the anal verge (anal orifice, anus) in the perineum below and the rectum above. Confusion and controversy exist regarding the anatomy of the anorectal region in anatomy and surgical texts. The description in this topic is from below upwards, as that is how this region is usually examined in clinical practice. Images depicting the anal canal can be seen below.[1, 2]
Coronal section of rectum and anal canal. Coronal section through the anal canal.
The pigmented, keratinized perianal skin of the buttocks (around the anal verge) has skin appendages (eg, hair, sweat glands, sebaceous glands); compare this with the anal canal skin above the anal verge, which is also pigmented and keratinized but does not have skin appendages.[3, 4]
In anatomy texts, the rectum changes to the anal canal at the dentate line. For surgeons, however, the demarcation between the rectum above and the anal canal below is the anorectal ring. The following is the description of the surgical anal canal (which in anatomical texts is described as the lower part of rectum).
The anal canal is completely extraperitoneal. The length of the (surgical) anal canal is about 4 cm (range, 3-5 cm), with two thirds of this being above the dentate line and one third below the dentate line (the anatomical anal canal).
The epithelium of the (anatomical) anal canal (between the anal verge below and the dentate line above) is variously described as anal mucosa or anal skin. The author believes that it should be called anal skin (anoderm), as it looks like (pigmented) skin, is sensitive like skin (why a fissure-in-ano is very painful), and is keratinized (but does not have skin appendages).
The dentate line (also called the pectinate line) is the site of fusion of the proctodeum below and the postallantoic gut above. It is a wavy demarcation formed by the anal valves (transverse folds of mucosa) at the inferior-most ends of the anal columns. Anal glands open above the anal valves into the anal crypts. The dentate line is not seen on inspection in

clinical practice, but under anesthesia the anal canal descends down, and the dentate line can be seen on slight retraction of the anal canal skin.
From a surgical perspective, the anal canal just above the dentate line for about 1-2 cm is called the transition zone. Beyond this transition zone, the (surgical) anal canal is lined with columnar epithelium (which is insensitive to cutting). Anal columns (of Morgagni) are 5-10 longitudinal (vertical) mucosal folds in the upper part of the anal canal.
At the bottom of these columns are anal crypts, or sinuses, into which open the anal glands and anal papillae. Infection of the anal glands is likely the initial event in causation of perianal abscess and fistula-in-ano. Three of these columns (left lateral, right posterior, and right anterior, at 3, 7, and 11 o’clock position in supine position) are prominent; they are called anal cushions and contain branches and tributaries of superior rectal (hemorrhoidal) artery and vein. When prominent, veins in these cushions form the internal hemorrhoids.
The anorectal ring is situated about 5 cm from anus. At the anorectal angle, the rectum turns backwards to continue as the anal canal.
Levator ani and coccygeus muscles form the pelvic diaphragm. Lateral to the anal canal are the pyramidal ischioanal (ischiorectal) fossae (1 on either side), below the pelvic diaphragm and above the perianal skin. The 2 ischioanal fossae communicate with each other behind the anal canal. The anterior relations of the anal canal are, in males, the seminal vesicles, prostate, and urethra, and, in females, the cervix and vagina with perineal body in between. In front of (anterior to) the anal canal is the rectovesical fascia (of Denonvilliers), and behind (posterior) is the presacral endopelvic fascia (of Waldeyer), under which lie a rich presacral plexus of veins. Posterior to the anal canal lie the tip of the coccyx (joined to it by the anococcygeal ligament) and lower sacrum.
Blood supply and lymphatics
The anal canal above the dentate line is supplied by the terminal branches of the superior rectal (hemorrhoidal) artery, which is the terminal branch of the inferior mesenteric artery. The middle rectal artery (a branch of the internal iliac artery) and the inferior rectal artery (a branch of the internal pudendal artery) supply the lower anal canal.
Underneath the anal canal skin (below the dentate line) lies the external hemorrhoidal plexus of veins, which drains into systemic veins. Underneath the anal canal mucosa (above dentate line) lies the internal hemorrhoidal plexus of veins, which drains into the portal system of veins. The anorectum is, therefore, an important area of portosystemic venous connection (the other being the esophagogastric junction). Lymphatics from the anal canal drain into the superficial inguinal group of lymph nodes.
Embryology
The anal canal below the dentate line develops from the proctodeum, while that above the dentate line develops from the endoderm of the hindgut.

Tissue, Nerves, and Muscles
The perianal skin is keratinized, stratified squamous epithelium with skin appendages (eg, hair, sweat glands, sebaceous glands, somatic nerve endings that are sensitive to pain). The (anatomical) anal canal skin (anoderm) is also keratinized, stratified squamous epithelium and has somatic nerve endings (sensitive to pain), but without skin appendages. The (surgical) anal canal mucosa is cuboidal in the transition zone and columnar above it; it is insensitive to pain. The rectal mucosa above the anorectal ring is lined by pinkish red, insensitive columnar epithelium.
The anorectal ring is formed by the puborectalis (the innermost fibers of levator ani muscle, which extends from the pubic bone, obturator fascia, and ischial spine to the coccyx and anococcygeal ligament) and the upper ends of the external and internal anal sphincters. Puborectalis plays a much more important role in continence than the internal and external sphincters. The involuntary autonomous internal anal sphincter is the lowermost continuation of the inner, circular smooth muscle layer of the rectum. The external longitudinal muscle layer continues as the corrugator cutis ani. The external anal sphincter has 3 parts: subcutaneous, superficial, and deep. The external anal sphincter is composed of skeletal muscle and is under voluntary control.
Pathophysiologic Variants
Pathophysiologic anal variants include the following:
Anal atresia Ectopic Anus Persistent Cloaca
Anal atresia (imperforate anus) is a low anorectal malformation in which the anus is either atretic (absent) or narrowed and the colon and rectum are normal. If the proctodeum and the postallantoic gut fail to unite, an imperforate anus results.
In ectopic anus, the anus is misplaced, usually anteriorly in the perineum (in males) or in the vagina (in females). Persistent cloaca, is a common passage in which lower GI tract (rectum), lower urinary tract (bladder or urethra), and lower genital tract in female (vagina) are open.
Perianal Lesions
The location of perianal lesions is described in relation to a clock (as seen in the supine position), eg, 2 o'clock, 7 o'clock. Sites of perianal lesions include the following:
Perianal skin – Abscess, hematoma (erroneously called thrombosed external hemorrhoids), external opening of fistula-in-ano, skin tag (in chronic fissure-in-ano)
Anal canal skin (anoderm, below dentate line) – Fissure-in-ano, external hemorrhoids, cancer
Anal canal mucosa (above dentate line) - Internal hemorrhoids, cancer

The dentate line cannot be felt on rectal examination but is seen on anoproctoscopy; under anesthesia, the dentate line can be seen on retraction of the perianal skin. The anorectal ring can be palpated on rectal examination (but not under anesthesia when the muscles relax).
Infection of an anal gland is considered the initial event in the formation of a perianal abscess and then fistula-in-ano. Fissure-in-ano is an ulcer in the sensitive anal canal skin and is a very painful condition. Fistula-in-ano can be intersphincteric, trans-sphincteric, or suprasphincteric. The internal opening of fistula-in-ano can be in the anal canal or rectum.
External hemorrhoids are in located below the dentate line on sensitive anal canal skin and are painful, while internal hemorrhoids are located above the dentate line in insensitive anal canal mucosa and are painless (unless complicated). For the same reason, internal hemorrhoids can be intervened (injected with sclerosant or ligated with rubber band) without anesthesia.
During posterior or lateral sphincterotomy for fissure in ano, it is only the internal sphincter that is divided.
A cruciate incision in the perianal skin lateral to the anal verge provides easy and direct access to ischiorectal fossae for drainage of an abscess.
Intersphincteric resection of the rectum (eg, for ulcerative colitis) follows the plane between the external and internal sphincters; external anal sphincter, levator ani, and puborectalis muscles are preserved.
In hand-sewn ileal pouch anal anastomosis (IPAA), also called restorative proctocolectomy (RPC) for ulcerative colitis, the ileal pouch is anastomosed to the dentate line, which is exposed perianally. For stapled IPAA, the surgical anal canal is divided 1-2 cm above the dentate line using a linear stapler; the ileal pouch is then anastomosed to the anal canal stump using a circular stapler.
Cancers of anal canal below the dentate line are usually squamous cell carcinoma (or basal cell carcinoma and melanoma), whereas those of the anal canal above dentate line (and of the rectum) are adenocarcinoma. Anal canal and low rectal cancers can infiltrate the anorectal ring and cause incontinence—a contraindication for sphincter preservation (by chemoradiotherapy for squamous cell carcinoma and low-anterior resection for adenocarcinoma). Anal canal cancer (or rectal cancer infiltrating into the anal canal) spreads to the inguinal lymph nodes.
Imaging considerations
Magnetic resonance imaging (MRI) has become the imaging modality of choice for delineation of anal and perianal anatomy in diseases such as fistula-in-ano and anorectal cancer, among others.
1. Agur AMR, Lee MJ, Grant JCB. Grant's Atlas of Anatomy. 10th Ed. London, UK: Lippincott Williams and Wilkins; 1999.
2. Sinnatamby CS. Last's Anatomy: Regional and Applied. 10th Ed. Edinburgh: Churchill Livingstone; 1999.

3. Romanes GJ. Thorax and Abdomen. In: Cunningham's Manual of Practical Anatomy. Vol II. 15th Ed. New York, NY: Medical Publications, Oxford University Press; 1986.
4. Gray H, Lewis WH. Gray's Anatomy of the Human Body. 20th ed. New York, NY: Bartleby; 2000:[Full Text].
5. Decker GAG, duPlassis. Lee McGregor's Synopsis of Surgcial Anatomy. Brsitol: John Wright and Sons.

BAHAN MEDSCAPE HEMORRHOID (http://emedicine.medscape.com/article/775407-overview)
Background
Hemorrhoids are swollen blood vessels in the lower rectum. They are among the most common causes of anal pathology, and subsequently are blamed for virtually any anorectal complaint by patients and medical professionals alike. Confusion often arises because the term "hemorrhoid" has been used to refer to both normal anatomic structures and pathologic structures. In the context of this article, "hemorrhoids" refers to the pathologic presentation of hemorrhoidal venous cushions.
Hemorrhoidal venous cushions are normal structures of the anorectum and are universally present unless a previous intervention has taken place. Because of their rich vascular supply, highly sensitive location, and tendency to engorge and prolapse, hemorrhoidal venous cushions are common causes of anal pathology.[1] Symptoms can range from mildly bothersome, such as pruritus, to quite concerning, such as rectal bleeding.
Vena hemorrhoidal bantal adalah normal struktur anorectum dan secara universal hadir kecuali suatu intervensi sebelumnya telah diambil tempat. Karena mereka kaya pasokan vaskular, sangat sensitif lokasi, dan kecenderungan untuk engorge dan prolapse, vena hemorrhoidal bantal yang umum menyebabkan patologi anal. 1 gejala dapat berkisar dari agak mengganggu, seperti pruritus, untuk cukup mengenai, seperti perdarahan dubur.
Although hemorrhoids are a common condition diagnosed in clinical practice, many patients are too embarrassed to ever seek treatment. Consequently, the true prevalence of pathologic hemorrhoids is not known.[2] In addition, although hemorrhoids are responsible for a large portion of anorectal complaints, it is important to rule out more serious conditions, such as other causes of gastrointestinal (GI) bleeding, before reflexively attributing symptoms to hemorrhoids.[3]
Meskipun wasir yang kondisi umum yang didiagnosis dalam kegiatan klinis, banyak pasien yang terlalu malu untuk pernah berobat. Akibatnya, prevalensi benar pathologic wasir tidak diketahui. 2 di samping itu meskipun wasir yang bertanggung jawab atas sebagian besar dari anorectal keluhan, merupakan hal yang penting untuk mengesampingkan lebih serius kondisi, seperti penyebab lain dari pencernaan ( gi ) berdarah, sebelum berkurangnya attributing gejala untuk wasir. 3
In a study of 198 physicians from different specialties, Grucela et al found the rate of correct identification for 7 common, benign anal pathologic conditions (including anal abscess, fissure, and fistula; prolapsed internal hemorrhoid; thrombosed external hemorrhoid; condyloma acuminata; and full-thickness rectal prolapse) was greatest for condylomata and rectal prolapse and was lowest for hemorrhoidal conditions.[4] There was no correlation between diagnostic accuracy and years of physician experience. The investigators found the overall diagnostic accuracy among the physicians to be 53.5%, with the accuracy for surgeons being 70.4% and that for the rest of the doctors being less than 50%.[4]

Dalam sebuah studi 198 dokter dari berbagai hale, grucela et al ditemukan tingkat benar identifikasi untuk 7 umum, jinak anal pathologic kondisi ( termasuk anal abses, fisura, dan fistula; prolapsed internal eksternal hemorrhoid; thrombosed hemorrhoid; condyloma acuminata; dan full-thickness dubur prolapse ) adalah terbesar untuk condylomata dan dubur prolapse dan terendah untuk hemorrhoidal kondisi. 4 tidak terdapat hubungan antara akurasi diagnostik dan tahun dari dokter pengalaman. Para peneliti tersebut menemukan keseluruhan akurasi diagnostik di antara dokter untuk menjadi 53.5 %, dengan keakuratan untuk ahli bedah yang 70.4 % dan bahwa untuk beristirahat dari para dokter yang kurang dari 50 %. 4
Historical note
Hemorrhoidal symptoms have historically been treated with dietary modifications, incantations, voodoo, quackery, and application of a hot poker. Molten lead has also been described as a treatment. The adverse effects of these treatments have a direct relationship to whether patients relay persistent or recurrent complaints to the clinician or return for further treatment.
Hemorrhoidal gejala telah secara historis diobati dengan modifikasi, makanan mantra-mantra, voodoo, perdukunan, dan penerapan panas poker. Cair memimpin juga telah dijelaskan sebagai pengobatan. Yang efek samping pengobatan ini memiliki sebuah hubungan langsung dengan apakah pasien relay persistent atau berulang keluhan ke clinician atau kembali untuk perawatan lebih lanjut.
Anatomy
Hemorrhoids are not varicosities; they are clusters of vascular tissue (eg, arterioles, venules, arteriolar-venular connections), smooth muscle (eg, Treitz muscle), and connective tissue lined by the normal epithelium of the anal canal. Hemorrhoids are present in utero and persist through normal adult life. Evidence indicates that hemorrhoidal bleeding is arterial and not venous. This evidence is supported by the bright red color and arterial pH of the blood.
Hemorrhoids are classified by their anatomic origin within the anal canal and by their position relative to the dentate line; thus, they are categorized into internal and external hemorrhoids (see the following image).
Wasir tidak varicosities; mereka kelompok pembuluh darah ( misalnya, arteriola, venula, arteriolar-venular koneksi ), otot halus ( misalnya, treitz otot ), dan jaringan ikat dibatasi oleh normal epitelium anal kanal. Wasir yang hadir di dalam rahim dan gigh melalui kehidupan dewasa. normal Bukti menunjukkan bahwa terjadinya pendarahan hemorrhoidal arteri dan tidak vena. Bukti ini didukung oleh arteri warna merah terang dan ph darah. Wasir yang diklasifikasikan oleh mereka asal dalam anatomi saluran dubur dan oleh mereka posisi relatif terhadap dentate garis; dengan demikian, mereka yang masuk ke internal dan eksternal wasir

Anatomy of external hemorrhoid. Image courtesy of MedicineNet, Inc.
External hemorrhoids develop from ectoderm and are covered by squamous epithelium, whereas internal hemorrhoids are derived from embryonic endoderm and lined with the columnar epithelium of anal mucosa. Similarly, external hemorrhoids are innervated by cutaneous nerves that supply the perianal area. These nerves include the pudendal nerve and the sacral plexus. Internal hemorrhoids are not supplied by somatic sensory nerves and therefore cannot cause pain. At the level of the dentate line, internal hemorrhoids are anchored to the underlying muscle by the mucosal suspensory ligament.
Eksternal wasir mengembangkan dari eksoderm dan yang ditutupi oleh skuamosa epitelium, sedangkan internal wasir yang berasal dari embrio endoderm dan dilapisi dengan kolumnar epitelium dari anal mukosa. Demikian pula, eksternal wasir yang diinervasi oleh saraf cornu yang memasok perianal wilayah. Saraf ini termasuk pudendal saraf dan pleksus sakralis. Internal wasir yang tidak disediakan oleh somatik saraf sensorik dan karena itu tidak bisa menyebabkan rasa sakit. Di tingkat dentate garis, internal wasir yang berlabuh untuk mendasari otot oleh mucosal suspensori ligamentum.
Hemorrhoidal venous cushions are a normal part of the human anorectum and arise from subepithelial connective tissue within the anal canal. Internal hemorrhoids have 3 main cushions, which are situated in the left lateral, right posterior (most common), and right anterior areas of the anal canal. However, this combination is found in only 19% of patients; hemorrhoids can be found at any position within the rectum. Minor tufts can be found between the major cushions.
Hemorrhoidal vena bantal adalah bagian normal manusia dan timbul dari subepithelial anorectum jaringan ikat di dalam kanal anus. Internal bantal, utama wasir memiliki 3 yang terletak di sebelah kiri lateralis, benar posterior ( yang paling umum ), dan kanan wilayah anterior kanal anus. Namun, kombinasi ini ditemukan di hanya 19 persen dari pasien; wasir dapat ditemukan di setiap posisi dalam rektum. Gumpalan kecil dapat ditemukan antara besar bantal.
Present in utero, these cushions surround and support distal anastomoses between the superior rectal arteries and the superior, middle, and inferior rectal veins. They also contain a subepithelial smooth muscle layer, contributing to the bulk of the cushions. Normal hemorrhoidal tissue accounts for approximately 15-20% of resting anal pressure and provides important sensory information, enabling the differentiation between solid, liquid, and gas.
External hemorrhoidal veins are found circumferentially under the anoderm; they can cause trouble anywhere around the circumference of the anus.

Hadir dalam rahim, bantal ini mengelilingi dan mendukung distal anastomoses antara arteri rektum superior dan unggul, tengah, dan vena rektal. Mereka juga mengandung lapisan subepithelial otot polos, memberikan kontribusi bagi sebagian besar bantal. Jaringan normal dalam sekitar 15-20% beristirahat anal tekanan dan menyediakan informasi sensorik yang penting, yang memungkinkan perbedaan antara padat, cair dan gas. Eksternal dalam vena ditemukan circumferentially di bawah anoderm; mereka dapat menyebabkan masalah di mana saja di sekitar lingkar anus.
Venous drainage of hemorrhoidal tissue mirrors embryologic origin. Internal hemorrhoids drain through the superior rectal vein into the portal system. External hemorrhoids drain through the inferior rectal vein into the inferior vena cava. Rich anastomoses exist between these 2 and the middle rectal vein, connecting the portal and systemic circulations.
Drainase vena dalam jaringan cermin asal-usul embryologic. Internal wasir mengalir melalui vena rektal unggul ke dalam sistem portal. Wasir eksternal mengalir melalui vena rektal inferior ke rendah vena cava. Kaya anastomoses ada antara ini 2 dan vena rektal tengah, menghubungkan portal dan sirkulasi sistemik.
Mixed hemorrhoids are confluent internal and external hemorrhoids.
Etiology and Pathophysiology
The term hemorrhoid is usually related to the symptoms caused by hemorrhoids. Hemorrhoids are present in healthy individuals. In fact, hemorrhoidal columns exist in utero. When these vascular cushions produce symptoms, they are referred to as hemorrhoids. Hemorrhoids generally cause symptoms when they become enlarged, inflamed, thrombosed, or prolapsed.
Istilah wasir biasanya berhubungan dengan gejala yang disebabkan oleh wasir. Wasir hadir pada individu yang sehat. Pada kenyataannya, dalam kolom berada dalam rahim. Ketika bantal vaskular ini menghasilkan gejala, mereka disebut sebagai wasir. Wasir umumnya menyebabkan gejala ketika mereka menjadi diperbesar, meradang, thrombosed, atau prolaps.
Most symptoms arise from enlarged internal hemorrhoids. Abnormal swelling of the anal cushions causes dilatation and engorgement of the arteriovenous plexuses. This leads to stretching of the suspensory muscles and eventual prolapse of rectal tissue through the anal canal. The engorged anal mucosa is easily traumatized, leading to rectal bleeding that is typically bright red due to high blood oxygen content within the arteriovenous anastomoses. Prolapse leads to soiling and mucus discharge (triggering pruritus) and predisposes to incarceration and strangulation.
Kebanyakan gejala yang timbul dari diperbesar internal wasir. Pembengkakan yang abnormal dari anal bantal menyebabkan dilatasi dan engorgement dari arteriovenous plexuses. Hal ini mengakibatkan peregangan dari suspensori otot dan akhirnya prolapse dari dubur jaringan melalui saluran dubur. Yang engorged anal mukosa adalah mudah trauma, yang mengarah ke dubur berdarah yang biasanya merah terang karena kadar oksigen darah tinggi dalam arteriovenous beranastomosis. Prolapse mengarah untuk mengotori dan cairan lendir ( memicu pruritus ) dan predisposes untuk penahanan dan pencekikan.

Although many patients and clinicians believe that hemorrhoids are caused by chronic constipation, prolonged sitting, and vigorous straining, little evidence to support a causative link exists. Some of these potential etiologies are briefly discussed below.
Kendati banyak pasien dan clinicians percaya bahwa wasir yang disebabkan oleh kronis sembelit, berkepanjangan duduk, dan kuat mengejan, sedikit bukti untuk mendukung causative link ada. Beberapa dari ini potensi etiologies yang sebentar dibahas di bawah
Decreased venous return penurunan aliran balik vena
Most authors agree that low-fiber diets cause small-caliber stools, which result in straining during defecation. This increased pressure causes engorgement of the hemorrhoids, possibly by interfering with venous return. Pregnancy and abnormally high tension of the internal sphincter muscle can also cause hemorrhoidal problems, presumably by means of the same mechanism, which is thought to be decreased venous return. Prolonged sitting on a toilet (eg, while reading) is believed to cause a relative venous return problem in the perianal area (a tourniquet effect), resulting in enlarged hemorrhoids. Aging causes weakening of the support structures, which facilitates prolapse. Weakening of support structures can occur as early as the third decade of life.
Kebanyakan penulis setuju bahwa diet rendah serat menyebabkan kaliber kecil tinja, yang mengakibatkan melelahkan saat buang air besar. Ini tekanan yang meningkat menyebabkan pembengkakan wasir, mungkin dengan ikut campur dengan vena kembali. Kehamilan dan abnormal tinggi ketegangan otot sfingter internal juga dapat menyebabkan masalah dalam, mungkin dengan menggunakan mekanisme yang sama, yang diperkirakan akan menurun vena kembali. Berkepanjangan duduk di toilet (misalnya, saat membaca) dipercayai menyebabkan relatif vena kembali masalah di daerah perianal (tourniquet efek), mengakibatkan wasir diperbesar. Penuaan menyebabkan melemahnya struktur dukungan, yang memfasilitasi prolaps. Pelemahan struktur dukungan dapat terjadi pada awal dekade ketiga kehidupan
Straining and constipation
Straining and constipation have long been thought of as culprits in the formation of hemorrhoids. This may or may not be true.[5, 6, 7] Patients who report hemorrhoids have a canal resting tone that is higher than normal. Of interest, the resting tone is lower after hemorrhoidectomy than it is before the procedure. This change in resting tone is the mechanism of action of Lord dilatation, a surgical procedure for anorectal complaints that is most commonly performed in the United Kingdom.
Tegang dan sembelit telah lama telah memikirkan seperti culprits dalam pembentukan wasir. Ini mungkin atau mungkin tidak menjadi kenyataan. 5, 6, 7 pasien yang melaporkan wasir telah sebuah kanal bertumpu nada yang lebih tinggi dari normal. Dari bunga, the bertumpu nada lebih rendah setelah hemorrhoidectomy dari itu adalah sebelum prosedur. Perubahan ini dalam bertumpu nada adalah mekanisme tindakan dari dilatasi, tuhan prosedur bedah untuk anorectal keluhan yang paling umum dilakukan di amerika kerajaan.
Pregnancy

Pregnancy clearly predisposes women to symptoms from hemorrhoids, although the etiology is unknown. Notably, most patients revert to their previously asymptomatic state after delivery. The relationship between pregnancy and hemorrhoids lends credence to hormonal changes or direct pressure as the culprit.
Portal hypertension and anorectal varices
Portal hypertension has often been mentioned in conjunction with hemorrhoids.[8, 9, 10]
However, hemorrhoidal symptoms do not occur more frequently in patients with portal hypertension than in those without it, and massive bleeding from hemorrhoids in these patients is unusual. Bleeding is very often complicated by coagulopathy. If bleeding is found, direct suture ligation of the offending column is suggested.
Hipertensi portal sering telah disebutkan dalam hubungannya dengan wasir. 8, 9, 10 namun, gejala hemorrhoidal tidak terjadi lebih sering dalam pasien dengan hipertensi daripada di portal orang-orang tanpa itu, dan besar pendarahan dari wasir dalam para pasien ini tidak biasa. Pendarahan ini sangat sering rumit oleh coagulopathy. Jika berdarah ini ditemukan, suture langsung ligation dari menyinggung kolom adalah menyarankan.
Anorectal varices are common in patients with portal hypertension.[11] Varices occur in the midrectum, at connections between the portal system and the middle and inferior rectal veins. Varices occur more frequently in patients who are noncirrhotic, and they rarely bleed. Treatment is usually directed at the underlying portal hypertension. Emergent control of bleeding can be obtained with suture ligation. Portosystemic shunts and transjugular intrahepatic portosystemic shunts (TIPS) have been used to control hypertension and thus, the bleeding.[12]
Anorectal varises yang umum pada pasien dengan hipertensi. portal 11 varises terjadi di midrectum, pada hubungan antara sistem portal dan tengah dan dubur veins. rendah Varises terjadi lebih sering pada pasien yang noncirrhotic, dan mereka jarang berdarah. Pengobatan biasanya diarahkan pada mendasari portal hipertensi. Emergent kontrol berdarah dapat diperoleh dengan jahitan ligation. Portosystemic shunts dan transjugular intrahepatic portosystemic shunts ( tips ) telah digunakan untuk mengontrol hipertensi dan dengan demikian, pendarahan. 12
Other risk factors
Other risk factors historically associated with the development of hemorrhoids include the following:
Lack of erect posture Familial tendency Higher socioeconomic status Chronic diarrhea Colon malignancy Hepatic disease Obesity Elevated anal resting pressure Spinal cord injury Loss of rectal muscle tone

Rectal surgery Episiotomy Anal intercourse Inflammatory bowel disease, including ulcerative colitis, and Crohn disease
Faktor risiko lain secara historis yang terkait dengan pengembangan wasir termasuk berikut: � kurangnya tegak postur � familial kecenderungan � status sosial ekonomi lebih tinggi kronis � diare � kolon keganasan penyakit hati � � obesitas � elevated anal beristirahat tekanan � cedera tulang belakang � hilangnya dubur otot � dubur operasi � episiotomy � anal seks � inflamasi penyakit usus, termasuk ulcerative colitis, dan crohn penyakit
Pathophysiology of symptoms of internal hemorrhoids
Internal hemorrhoids cannot cause cutaneous pain, because they are above the dentate line and are not innervated by cutaneous nerves. However, they can bleed, prolapse, and, as a result of the deposition of an irritant onto the sensitive perianal skin, cause perianal itching and irritation. Internal hemorrhoids can produce perianal pain by prolapsing and causing spasm of the sphincter complex around the hemorrhoids. This spasm results in discomfort while the prolapsed hemorrhoids are exposed. This muscle discomfort is relieved with reduction.
Wasir internal tidak menyebabkan kulit sakit, karena mereka di atas garis gyrus dan tidak dipersarafi oleh saraf Cornu. Namun, mereka dapat berdarah, prolaps dan, sebagai akibat dari pengendapan iritan ke kulit sensitif perianal, menyebabkan perianal gatal dan iritasi. Wasir internal dapat menghasilkan rasa sakit perianal dengan prolapsing dan menyebabkan kejang sfingter kompleks di sekitar wasir. Kejang ini mengakibatkan ketidaknyamanan sementara wasir prolaps yang terkena. Ketidaknyamanan otot ini adalah lega dengan pengurangan.
Internal hemorrhoids can also cause acute pain when incarcerated and strangulated. Again, the pain is related to the sphincter complex spasm. Strangulation with necrosis may cause more deep discomfort. When these catastrophic events occur, the sphincter spasm often causes concomitant external thrombosis. External thrombosis causes acute cutaneous pain. This constellation of symptoms is referred to as acute hemorrhoidal crisis and usually requires emergent treatment.
Wasir internal juga dapat menyebabkan nyeri akut ketika dipenjara dan strangulated. Sekali lagi, rasa sakit berhubungan dengan kejang sfingter kompleks. Pencekikan dengan nekrosis dapat menyebabkan ketidaknyamanan lebih mendalam. Ketika terjadi peristiwa bencana, kejang sfingter sering menyebabkan seiring eksternal trombosis. Eksternal trombosis menyebabkan sakit kulit akut. Rasi bintang ini gejala dirujuk sebagai krisis dalam akut dan biasanya membutuhkan perawatan yang muncul.
Internal hemorrhoids most commonly cause painless bleeding with bowel movements. The covering epithelium is damaged by the hard bowel movement, and the underlying veins bleed. With spasm of the sphincter complex elevating pressure, the internal hemorrhoidal veins can spurt.
Internal hemorrhoids can deposit mucus onto the perianal tissue with prolapse. This mucus with microscopic stool contents can cause a localized dermatitis, which is called pruritus ani.

Generally, hemorrhoids are merely the vehicle by which the offending elements reach the perianal tissue. Hemorrhoids are not the primary offenders.
Wasir internal paling sering menyebabkan perdarahan menyakitkan dengan gerakan usus. Epitel meliputi rusak oleh gerakan usus yang keras, dan vena mendasari berdarah. Dengan kejang sfingter kompleks mengangkat tekanan, internal dalam vena dapat menyembur. Internal wasir bisa deposit lendir ke jaringan perianal dengan prolaps. Lendir ini dengan bangku mikroskopis isi dapat menyebabkan dermatitis lokal, yang disebut gatal ani. Secara umum wasir adalah hanya kendaraan yang menyinggung elemen mencapai jaringan perianal. Wasir adalah tidak pelaku utama.
Pathophysiology of symptoms of external hemorrhoids
External hemorrhoids cause symptoms in 2 ways. First, acute thrombosis of the underlying external hemorrhoidal vein can occur. Acute thrombosis is usually related to a specific event, such as physical exertion, straining with constipation, a bout of diarrhea, or a change in diet. These are acute, painful events.
Eksternal wasir menyebabkan gejala dalam 2 cara. Pertama, akut trombosis mendasari eksternal hemorrhoidal vena dapat terjadi. Akut biasanya terkait dengan trombosis jgs, tertentu seperti tenaga fisik, tegang dengan sembelit, serangan diare, atau perubahan dalam diet. Ini adalah akut, menyakitkan peristiwa.
Pain results from rapid distention of innervated skin by the clot and surrounding edema. The pain lasts 7-14 days and resolves with resolution of the thrombosis. With this resolution, the stretched anoderm persists as excess skin or skin tags. External thromboses occasionally erode the overlying skin and cause bleeding. Recurrence occurs approximately 40-50% of the time, at the same site (because the underlying damaged vein remains there). Simply removing the blood clot and leaving the weakened vein in place, rather than excising the offending vein with the clot, will predispose the patient to recurrence.
Rasa sakit hasil dari distensi cepat kulit diinervasi oleh bekuan dan sekitarnya edema. Rasa sakit berlangsung 7-14 hari dan memutuskan: dengan resolusi tentang masalah-masalah. trombosis Dengan resolusi ini, membentang anoderm tersebut bertahan sebagai kelebihan kulit atau kulit tag. Thromboses eksternal kadang-kadang mengikis the overlying kulit dan menyebabkan berdarah. Kambuh terjadi sekitar 40-50 % dari waktu, pada saat yang sama situs ( karena para yang mendasari vena yang rusak tetap sana ). Hanya menghapus darah menggumpal dan meninggalkan melemah pembuluh darah di tempat, daripada excising the menyinggung pembuluh darah dengan bekuan, akan mempengaruhi pasien untuk kambuh.
External hemorrhoids can also cause hygiene difficulties, with the excess, redundant skin left after an acute thrombosis (skin tags) being accountable for these problems. External hemorrhoidal veins found under the perianal skin obviously cannot cause hygiene problems; however, excess skin in the perianal area can mechanically interfere with cleansing.
Wasir eksternal juga dapat menyebabkan kesulitan kebersihan, dengan berlebihan, kelebihan kulit yang tersisa setelah trombosis akut (kulit Tag) yang bertanggung jawab untuk masalah ini. Eksternal dalam vena yang ditemukan di bawah kulit perianal jelas tidak menyebabkan masalah kebersihan; Namun, kelebihan kulit di daerah perianal dapat mekanis mengganggu pembersihan.

Epidemiology
Worldwide, the prevalence of symptomatic hemorrhoids is estimated at 4.4% in the general population. In the United States, up to one third of the 10 million people with hemorrhoids seek medical treatment, resulting in 1.5 million related prescriptions per year.
The number of hemorrhoidectomies performed in US hospitals is declining. A peak of 117 hemorrhoidectomies per 100,000 people was reached in 1974; this rate declined to 37 hemorrhoidectomies per 100,000 people in 1987. Outpatient and office treatment of hemorrhoids account for some of this decline.
Di dunia, prevalensi gejala wasir diperkirakan 4.4 % di populasi umum. Di amerika serikat, hingga sepertiga dari 10 juta orang dengan wasir mencari pengobatan medis, mengakibatkan 1,5 juta terkait resep per tahun. Jumlah hemorrhoidectomies dilakukan di rumah sakit kita justru mengalami penurunan. Puncak dari 117 hemorrhoidectomies per 100.000 orang itu dicapai pada tahun 1974; angka ini menurun menjadi 37 hemorrhoidectomies per 100.000 orang pada tahun 1987. Rawat jalan dan kantor pengobatan wasir account untuk melakukan hal tersebut menurun
Patients presenting with hemorrhoidal disease are more frequently white, from higher socioeconomic status, and from rural areas. There is no known sex predilection, although men are more likely to seek treatment. However, pregnancy causes physiologic changes that predispose women to developing symptomatic hemorrhoids. As the gravid uterus expands, it compresses the inferior vena cava, causing decreased venous return and distal engorgement.
External hemorrhoids occur more commonly in young and middle-aged adults than in older adults. The prevalence of hemorrhoids increases with age, with a peak in persons aged 45-65 years.
Pasien menyajikan dengan hemorrhoidal penyakit lebih sering putih, dari status sosial ekonomi lebih tinggi, dan dari daerah pedesaan. Ada kecenderungan, seks tidak dikenal meskipun pria lebih mungkin untuk mencari pengobatan. Namun, kehamilan menyebabkan physiologic perubahan yang mempengaruhi wanita untuk mengembangkan gejala wasir. Sebagai hypnose rahim memperluas, itu kompres kava inferior, menyebabkan penurunan vena distal kembali dan engorgement. Wasir eksternal terjadi lebih sering dalam muda dan orang dewasa setengah baya dewasa yang lebih tua daripada di. Prevalensi wasir meningkat dengan usia, dengan puncak pada orang berusia 45-65 tahun
Prognosis
Most hemorrhoids resolve spontaneously or with conservative medical therapy alone. However, complications can include thrombosis, secondary infection, ulceration, abscess, and incontinence. The recurrence rate with nonsurgical techniques is 10-50% over a 5-year period, whereas that of surgical hemorrhoidectomy is less than 5%.
Regarding complications from surgery, well-trained surgeons should experience complications in fewer than 5% of cases. Complications include stenosis, bleeding, infection, recurrence, nonhealing wounds, and fistula formation. Urinary retention is directly related to

the anesthetic technique used and to the perioperative fluids administered. Limiting fluids and the routine use of local anesthesia can reduce urinary retention to less than 5%.
Kebanyakan wasir menyelesaikan secara spontan atau dengan terapi medis konservatif sendirian. Namun, komplikasi dapat mencakup trombosis, infeksi sekunder, ulserasi, abses, dan inkontinensia. Tingkat kekambuhan dengan teknik non-bedah adalah 10-50% selama 5 tahun periode, sedangkan yang metode bedah kurang dari 5%. Mengenai komplikasi dari operasi, ahli bedah terlatih harus mengalami komplikasi dalam kurang dari 5% dari kasus. Komplikasi termasuk stenosis, perdarahan, infeksi, kambuh, nonhealing luka dan fistula pembentukan. Retensi urin terkait langsung dengan teknik anestesi yang digunakan dan untuk pemberian cairan yang diberikan. Membatasi cairan dan penggunaan rutin anestesi lokal dapat mengurangi retensi urin untuk kurang dari 5%
History
Most laypersons and many practitioners attribute all perianal symptoms to hemorrhoids. The astute clinician can often listen to a patient's description of symptoms and ascertain the source of the problem or condition before confirmatory examination. Nonhemorrhoidal causes of symptoms (eg, fissure, abscess, fistula, pruritus ani, condylomata, and viral or bacterial skin infection) need to be excluded.
The most common presentation of hemorrhoids is rectal bleeding, pain, pruritus, or prolapse. Because these symptoms are extremely nonspecific and may be seen in a number of anorectal diseases, the physician must therefore rely on a thorough history to help narrow the differential diagnosis and must perform an adequate physical examination (including anoscopy when indicated) to confirm the diagnosis.
Kebanyakan laypersons dan banyak praktisi atribut semua perianal Gejala wasir. Klinisi cerdik dapat sering mendengarkan keterangan pasien gejala dan memastikan sumber masalah atau kondisi sebelum pemeriksaan konfirmasi. Nonhemorrhoidal penyebab gejala (misalnya, fisura, abses, fistula, gatal ani, condylomata, dan infeksi virus atau bakteri kulit) harus dikecualikan. Presentasi yang paling umum wasir adalah rektal berdarah, sakit, gatal atau prolaps. Karena gejala-gejala ini sangat spesifik dan dapat dilihat di sejumlah penyakit anorectal, dokter karena itu harus mengandalkan sejarah yang menyeluruh untuk membantu mempersempit diagnosis diferensial dan harus melakukan pemeriksaan fisik memadai (termasuk anoscopy ketika ditunjukkan) untuk mengonfirmasikan diagnosis.
Familial predisposition, diet, a history of constipation or diarrhea, and a history of prolonged sitting or heavy lifting are also relevant, as are weight loss, abdominal pain, or any change in appetite or bowel habits. The presence of pruritus or any discharge should also be noted.
Inflammatory bowel diseases (eg, ulcerative colitis, Crohn disease) need to be ruled out as the cause of symptoms. Human immunodeficiency virus (HIV) infection and other immunosuppressive diseases can also alter treatment plans.
Familial kecenderungan, diet, sejarah sembelit atau diare, dan sejarah lama duduk atau angkat berat juga relevan, seperti berat badan, sakit perut atau perubahan dalam kebiasaan nafsu makan atau usus. Kehadiran gatal atau pelepasan apapun juga harus dicatat. Penyakit inflamasi usus (misalnya, kolitis ulseratif, penyakit Crohn) perlu dapat dikesampingkan

sebagai penyebab gejala. Human immunodeficiency virus HIV infeksi dan penyakit lainnya imunosupresif juga dapat mengubah rencana pengobatan.
Symptoms
An adequate history should include the onset and duration of symptoms. In addition to characterizing any pain, bleeding, protrusion, or change in bowel habits, special attention should be placed on the patient's coagulation history and immune status.
Rectal bleeding is the most common presenting symptom. The blood is usually bright red and may drip, squirt into the toilet bowl, or appear as streaks on the toilet paper. The physician should inquire about the quantity, color, and timing of any rectal bleeding. Darker blood or blood mixed with stool should raise suspicion of a more proximal cause of bleeding.
Sejarah yang memadai harus mencakup onset dan durasi gejala. Selain mencirikan sakit, perdarahan, tonjolan, atau perubahan kebiasaan buang air besar, perhatian khusus harus ditempatkan pada status pasien koagulasi sejarah dan kekebalan tubuh. Perdarahan rektal adalah paling umum gejalanya presentasi. Darah merah biasanya cerah dan mungkin menetes, muncrat ke dalam mangkuk toilet, atau muncul sebagai garis-garis kertas toilet. Dokter harus menanyakan tentang kuantitas, warna, dan waktu perdarahan rektal apapun. Gelap darah atau darah yang dicampur dengan bangku harus meningkatkan kecurigaan lebih proksimal penyebab pendarahan
A patient with a thrombosed external hemorrhoid may present with complaints of an acutely painful mass at the rectum (see the image below). Pain truly caused by hemorrhoids usually arises only with acute thrombus formation. This pain peaks at 48-72 hours and begins to decline by the fourth day as the thrombus organizes. New-onset anal pain in the absence of a thrombosed hemorrhoid should prompt investigation for an alternate cause, such as an intersphincteric abscess or anal fissure. As many as 20% of patients with hemorrhoids will have concomitant anal fissures.
Pasien dengan thrombosed eksternal wasir mungkin hadir dengan keluhan massa akut menyakitkan di dubur (Lihat gambar di bawah). Sakit benar-benar disebabkan oleh wasir biasanya timbul hanya dengan pembentukan trombus akut. Rasa sakit ini puncak pada 48-72 jam dan mulai menurun pada hari keempat sebagai trombus menyelenggarakan. Onset baru anal rasa sakit dalam ketiadaan wasir thrombosed harus meminta penyelidikan untuk tujuan alternatif, seperti abses intersphincteric atau anal retakan. Sebanyak 20% pasien dengan wasir akan memiliki seiring anal retakan
Thrombosed hemorrhoid. This hemorrhoid was treated by incision and removal of clot.

The presence, timing, and reducibility of prolapse, when present, will help classify the grade of internal hemorrhoids and guide the therapeutic approach (see Grading of Internal Hemorrhoids). Grade I internal hemorrhoids are usually asymptomatic but, at times, may cause minimal bleeding. Grades II, III, or IV internal hemorrhoids usually present with painless bleeding but also may present with complaints of a dull aching pain, pruritus, or other symptoms due to prolapse.
Kehadiran, waktu, dan reducibility prolaps, ketika hadir, akan membantu mengklasifikasikan kelas internal wasir dan panduan terapi pendekatan (Lihat Grading wasir Internal). Kelas saya wasir internal biasanya asimtomatik, tapi kadang-kadang, dapat menyebabkan perdarahan yang minimal. Kelas II, III atau IV wasir internal biasanya ditandai dengan adanya perdarahan yang menyakitkan tetapi juga dapat hadir dengan keluhan nyeri ngilu, gatal atau gejala lain karena untuk prolaps.
Physical Examination
In addition to the general physical examination, physicians should also perform visual inspection of the rectum, digital rectal examination, and anoscopy or proctosigmoidoscopy when appropriate.
The preferred position for the digital rectal examination is the left lateral decubitus with the patient's knees flexed toward the chest. Topical anesthetics (eg, 20% benzocaine or 5% lidocaine ointment) may help to reduce any discomfort caused by examination.
Inspect and examine the entire perianal area. Warn the patient before any probing or poking. Because patient apprehension is great before any anal examination, go to great lengths to reassure the patient. Gentle spreading of the buttocks allows easy visualization of most of the anoderm; this includes the distal anal canal. Anal fissures and perianal dermatitis (pruritus ani) are easily visible without internal probing. Note the location and size of skin tags and the presence of thromboses. Normal corrugation of the anoderm and a normal anal wink with stimulation confirms intact sensation.
Selain pemeriksaan fisik umum, dokter harus juga melakukan inspeksi visual rektum, digital pemeriksaan dubur, dan anoscopy atau proctosigmoidoscopy saat yang tepat. Posisi yang lebih disukai untuk digital pemeriksaan dubur adalah DEKUBITUS lateral kiri dengan pasien lutut tertekuk ke arah dada. Anestesi topikal (misalnya, 20% benzokain atau 5% lidokain salep) dapat membantu untuk mengurangi rasa nyeri yang disebabkan oleh pemeriksaan. Memeriksa dan memeriksa daerah seluruh perianal. Memperingatkan pasien sebelum menyelidik atau menusuk. Karena pasien ketakutan besar sebelum pemeriksaan dubur apapun, berusaha keras untuk meyakinkan pasien. Penyebaran lembut pantat memungkinkan mudah visualisasi dari sebagian besar anoderm; ini termasuk distal anus. Anal retakan dan dermatitis perianal (gatal ani) yang mudah terlihat tanpa penyelidikan internal. Catatan lokasi dan ukuran kulit tag dan kehadiran thromboses. Normal kerut anoderm dan normal Wink anal dengan stimulasi menegaskan utuh sensasi.
The following are external findings that are important to note:
Redundant tissue Skin tags from old thrombosed external hemorrhoids Fissures

Fistulas Signs of infection or abscess formation Rectal or hemorrhoidal prolapse, appearing as a bluish, tender perianal mass
Digital examination of the anal canal can identify any indurated or ulcerated areas. Also assess for any masses, tenderness, mucoid discharge or blood, and rectal tone. Be sure to palpate the prostate in all men. Because internal hemorrhoids are soft vascular structures, they are usually not palpable unless thrombosed.
Berikut ini adalah temuan eksternal yang penting untuk dicatat: � jaringan berlebihan � tag kulit dari lama thrombosed wasir � eksternal celah � fistulas tanda-tanda � dari infeksi atau pembentukan abses � atau hemorrhoidal dubur prolapse, muncul sebagai sebuah kebiruan, perianal tender massal pemeriksaan digital saluran dubur dapat mengidentifikasi salah satu indurated atau ulcerated daerah. Juga menilai untuk setiap massa, kelembutan, debit kental yang atau darah, dan dubur nada. Pastikan untuk palpate prostat dalam semua orang. Karena wasir internal yang lembut struktur vaskular, mereka biasanya tidak teraba kecuali thrombosed
Current guidelines from most gastrointestinal and surgical societies advocate anoscopy and/or flexible sigmoidoscopy to evaluate any bright-red rectal bleeding. Colonoscopy should be considered in the evaluation of any rectal bleeding that is not typical of hemorrhoids such as in the presence of strong risk factors for colonic malignancy or in the setting of rectal bleeding with a negative anorectal examination.
Saat ini petunjuk dari yang paling pencernaan dan bedah masyarakat menadvokasi anoscopy dan / atau fleksibel sigmoidoscopy untuk mengevaluasi setiap bright-red dubur berdarah. Kolonoskopi harus dipertimbangkan dalam evaluasi setiap dubur pendarahan yang tidak khas dari wasir seperti di hadapan kuat faktor resiko bagi colonic penyakit berbahaya atau dalam pengaturan dari dubur pendarahan dengan negatif anorectal pemeriksaan.
Grading of Internal Hemorrhoids
Most clinicians use the grading system proposed by Banov et al in 1985, which classifies internal hemorrhoids by their degree of prolapse into the anal canal. This system both correlates with symptoms and guides therapeutic approaches, as follows.
Grade I hemorrhoids project into the anal canal and often bleed but do not prolapse Grade II hemorrhoids may protrude beyond the anal verge with straining or defecating but
reduce spontaneously when straining ceases (ie, return to their resting point by themselves) Grade III hemorrhoids protrude spontaneously or with straining and require manual
reduction (ie, require manual effort for replacement into the anal canal) Grade IV hemorrhoids chronically prolapse and cannot be reduced; these lesions usually
contain both internal and external components and may present with acute thrombosis or strangulation
Paling clinicians menggunakan sistem grading diusulkan oleh banov et al pada tahun 1985, internal mana mengklasifikasikan wasir oleh mereka gelar dari prolapse ke dalam anal kanal. Sistem ini kedua berkorelasi dengan gejala pendekatan terapi dan panduan, seperti berikut. Kelas � aku wasir proyek ke kanal anus dan sering berdarah tapi tidak prolapse � grade ii wasir dapat dibenamkan di luar verge anal dengan tegang atau buang air besar tapi

mengurangi secara spontan ketika tegang berhenti ( ie, kembali ke beristirahat mereka titik dengan diri mereka sendiri ) � grade iii wasir menonjol secara spontan atau dengan tegang dan memerlukan pengurangan manual ( ie, memerlukan upaya untuk manual penggantian ke dalam kanal anal ) � iv grade wasir kronis prolapse dan tidak dapat dikurangi; luka-luka ini biasanya berisi keduanya komponen internal dan eksternal dan dapat hadir dengan trombosis akut atau pencekikan
Diagnostic Considerations
Hemorrhoidal complaints are usually not associated with other medical conditions or diseases. However, patients with the following diseases and conditions have an increased risk of hemorrhoidal complaints:
Inflammatory bowel disease (IBD): IBD and hemorrhoidal problems occur frequently; unusual hemorrhoidal presentations and findings should alert the clinician to the potential of IBD.
Ulcerative colitis and Crohn disease Pregnancy
Varicosities caused from portal hypertension are a distinct entity from hemorrhoids.
Other conditions that should be considered when evaluating a patient with suspected hemorrhoids include anal cancer, anal fissures, and anal fistulae; pedunculated polyps; perianal abscesses; pruritus ani; and colorectal tumors.
Keluhan hemorrhoidal yang biasanya tidak terkait dengan kondisi medis lainnya atau penyakit. Namun, pasien dengan penyakit berikut dan kondisi memiliki sebuah peningkatan risiko dari hemorrhoidal keluhan: � usus inflamasi penyakit ( ibd ): ibd hemorrhoidal dan terjadi permasalahan sering; tidak biasa presentasi hemorrhoidal dan temuan harus aiert tersebut clinician untuk potensi dari ibd. � ulcerative colitis dan penyakit crohn kehamilan � varicosities yang disebabkan dari hipertensi portal apakah sebuah entitas yang berbeda dari wasir. Kondisi lain yang harus dianggap ketika mengevaluasi pasien dengan dugaan wasir termasuk kanker anal, fissures, anal dan anal; pedunkulata fistulae polip; perianal abses; pruritus ani; dan tumor kolorektal
Differential Diagnoses
Condyloma Acuminata Proctitis Rectal Prolapse
Approach Considerations
Most gastrointestinal and surgical societies advocate anoscopy and/or flexible sigmoidoscopy to evaluate any bright-red rectal bleeding. Colonoscopy should be considered in the evaluation of any rectal bleeding that is not typical of hemorrhoids such as in the presence of strong risk factors for colonic malignancy or in the setting of rectal bleeding with a negative anorectal examination.

Pertimbangan pendekatan yang paling pencernaan dan bedah masyarakat menadvokasi anoscopy dan / atau fleksibel sigmoidoscopy untuk mengevaluasi setiap bright-red dubur berdarah. Kolonoskopi harus dipertimbangkan dalam evaluasi setiap dubur pendarahan yang tidak khas dari wasir seperti di hadapan faktor risiko yang kuat untuk colonic keganasan atau dalam pengaturan dubur pendarahan dengan negatif anorectal pemeriksaan.
Hematologic Tests
A complete blood cell (CBC) count may be useful as a marker for infection. Anemia due to hemorrhoidal bleeding is possible,[3] albeit rare (0.5 cases per 100,000 patients), and its presence should raise suspicion of an alternate diagnosis. Hematocrit testing is suggested if excessive bleeding with concomitant anemia is suspected.
Coagulation studies are indicated if the history and physical examination suggest coagulopathy.
Penghitungan sel darah lengkap (CBC) mungkin berguna sebagai penanda untuk infeksi. Anemia karena pendarahan dalam muka, [3] Meskipun langka (0.5 kasus per 100.000 pasien), dan kehadirannya harus meningkatkan kecurigaan diagnosis alternatif. Pengujian hematokrit disarankan jika perdarahan yang berlebihan dengan anemia seiring diduga. Koagulasi penelitian menunjukkan jika sejarah dan pemeriksaan fisik menyarankan koagulopati.
Anoscopy and Flexible Sigmoidoscopy
Anoscopy is mandatory for viewing internal hemorrhoids. The anoscope should be a side-viewing one. When angled well by the examiner, the side-viewing anoscope allows the soft hemorrhoidal tufts to fill the beveled end of the scope and to be appropriately evaluated. Prolapse can be observed when the patient performs a Valsalva maneuver.
Flexible sigmoidoscopy is performed to exclude proximal disease. Having a patient strain while sitting on a toilet may reproduce prolapse most accurately; in addition, examining patients while they sit on a toilet can be very helpful in indeterminate cases.
Anoscopy adalah wajib untuk melihat internal wasir. Yang anoscope harus bisa menjadi side-viewing satu. Ketika siku dengan baik oleh ditail, yang side-viewing anoscope memungkinkan lembut hemorrhoidal jumbai miring untuk mengisi bagian ujung ruang lingkup dan harus tepat evaluasi. Prolapse dapat diamati ketika pasien melakukan manuver. valsava Fleksibel sigmoidoscopy dilakukan untuk mengecualikan proksimal penyakit. Memiliki seorang pasien ketegangan sambil duduk di toilet dapat bereproduksi prolapse yang paling akurat; di samping itu memeriksa pasien sementara mereka duduk di toilet bisa sangat membantu dalam tak tentu kasus.
Other Diagnostic Imaging Studies
Proctoscopy may be performed to supplement anoscopy, and proctography may be indicated in rectal prolapse.

Colonoscopy, virtual colonoscopy, and barium enema are reserved for cases of bleeding without an identified anal source. These symptoms are not attributable to hemorrhoids and are considered to be non–outlet-type bleeding. Barium enema study or virtual colonoscopy is also suggested if proximal colonic and intestinal diseases must be excluded and if endoscopy is not helpful.
Full evaluation of the large bowel with colonoscopy is recommended for patients with significant abdominal symptoms, weight loss, change in bowel habits, age older than 50 years, or other risk factors for colonic malignancy.
Proctoscopy dapat dilakukan untuk melengkapi anoscopy, dan proctography dapat ditunjukkan di dubur prolapse. Kolonoskopi, kolonoskopi virtual, dan barium enema diperuntukkan bagi kasus berdarah tanpa sebuah diidentifikasi anal sumber. Gejala ini tidak berkaitan dengan wasir dan dianggap non � outlet-type berdarah. Barium enema studi kolonoskopi atau virtual juga disarankan jika colonic proksimal dan penyakit usus harus dikeluarkan dan jika endoskopi tidak membantu. Penuh evaluasi kolonoskopi usus besar dengan disarankan untuk pasien dengan gejala, abdominalis signifikan penurunan berat badan, perubahan kebiasaan, usus usia lebih tua dari 50 tahun, atau faktor risiko lain untuk colonic keganasan
Histologic Features
Routine histologic examination of hemorrhoidal tissue is usually unrewarding, especially if it is grossly examined by an experienced anorectal surgeon. Any suspicious tissue must be sent for microscopic evaluation. External hemorrhoids are classified by the underlying pathology and symptoms, which include thrombosed veins, bleeding from eroded blood clots, and skin tags causing hygiene problems.
Pemeriksaan histologis rutin dalam jaringan biasanya unrewarding, terutama jika itu terlalu dikaji oleh seorang ahli bedah berpengalaman anorectal. Jaringan mencurigakan apapun harus dikirim untuk evaluasi mikroskopis. Wasir eksternal diklasifikasikan oleh mendasari patologi dan gejala, yang meliputi vena thrombosed, perdarahan dari gumpalan darah yang terkikis, dan skin tag yang menyebabkan masalah kebersihan
Approach Considerations
Treat hemorrhoids only when the patient complains of them. The old adage that it is hard to make an asymptomatic patient better applies here. No matter how bad the hemorrhoids look to the practitioner, they should not be treated unless they bother the patient.
Treatment of hemorrhoids is divided by the cause of symptoms, into internal and external treatments. Accurately classifying a patient's symptoms and the relation of the symptoms to internal and external hemorrhoids is important.
Mengobati wasir hanya ketika pasien mengeluh mereka. Pepatah lama sulit untuk membuat pasien asimtomatik lebih berlaku di sini. Tidak peduli seberapa buruk wasir melihat ke praktisi, mereka tidak boleh diperlakukan kecuali mereka mengganggu pasien. Pengobatan wasir terbagi oleh penyebab gejala, pengobatan internal dan eksternal. Akurat

mengklasifikasikan pasien gejala dan hubungan antara gejala wasir internal dan eksternal penting.
Internal hemorrhoids
Internal hemorrhoids do not have cutaneous innervation and can therefore be destroyed without anesthetic, and the treatment may be surgical or nonsurgical. Internal hemorrhoid symptoms often respond to increased fiber and liquid intake and to avoidance of straining and prolonged toilet sitting. Nonoperative therapy works well for symptoms that persist despite the use of conservative therapy. Most nonsurgical procedures currently available are performed in the clinic or ambulatory setting.
The following is a quick summary of treatment for internal hemorrhoids by grade:
Wasir internal tidak memiliki kulit persarafan dan karena itu dapat dihancurkan tanpa anestesi, dan pengobatan mungkin pembedahan atau non-bedah. Gejala-gejala wasir internal sering menanggapi serat meningkat dan asupan cairan dan menghindari melelahkan dan berkepanjangan toilet duduk. Terapi non-operatif bekerja dengan baik untuk gejala yang bertahan meskipun penggunaan terapi konservatif. Kebanyakan prosedur non-bedah yang tersedia saat ini dilakukan di klinik atau Ambulatori pengaturan. Berikut ini adalah ringkasan dari perawatan untuk internal wasir oleh kelas:
Grade I hemorrhoids are treated with conservative medical therapy and avoidance of nonsteroidal anti-inflammatory drugs (NSAIDs) and spicy or fatty foods
Grade II or III hemorrhoids are initially treated with nonsurgical procedures Very symptomatic grade III and grade IV hemorrhoids are best treated with surgical
hemorrhoidectomy Treatment of grade IV internal hemorrhoids or any incarcerated or gangrenous tissue
requires prompt surgical consultation
Stapled hemorrhoid surgery, or procedure for prolapsing hemorrhoids (PPH), is an excellent alternative for treating internal hemorrhoids that have not been amenable to conservative or nonoperative approaches. Short- and medium-term results are excellent. Patients with minimal external tags and large internal hemorrhoids are easily treated with procedure for prolapsing hemorrhoids and skin tag excision. Operative resection is sometimes required to control the symptoms of internal hemorrhoids.
kelas aku wasir dirawat dengan terapi medis konservatif dan menghindari obat anti-inflamasi nonsteroid ( nsaids ) dan makanan berlemak atau pedas � kelas ii atau iii wasir yang awalnya diperlakukan dengan prosedur nonsurgical � sangat gejala kelas iii dan kelas iv wasir yang terbaik diperlakukan dengan bedah hemorrhoidectomy kelas iv internal � pengobatan wasir atau setiap sepenjaraku jaringan atau gangrenous memerlukan prompt bedah konsultasi stapled hemorrhoid operasi, atau prosedur untuk prolapsing wasir ( pph ), yang sangat bagus untuk pengobatan alternatif internal wasir yang belum setuju untuk konservatif atau nonoperative mendekati. Pendek - dan jangka menengah. hasil yang sangat baik Pasien dengan tag eksternal dan internal minimal besar wasir yang mudah diperlakukan dengan prosedur untuk prolapsing wasir dan kulit sentuh-sentuhan eksisi. Operasi reseksi kadang-kadang diperlukan untuk mengontrol gejala internal wasir.
External hemorrhoids

External hemorrhoid symptoms are generally divided into problems with acute thrombosis and hygiene/skin tag complaints. The former respond well to office excision (not enucleation), whereas operative resection is reserved for the latter. Remember that therapy is directed solely at the symptoms, not at aesthetics.
When performed well, operative hemorrhoidectomy should have a 2-5% recurrence rate. Nonoperative techniques, such as rubber band ligation, produce recurrence rates of 30-50% within 5-10 years. However, these recurrences can usually be addressed with further nonoperative treatments.[13] Long-term results from procedure for prolapsing hemorrhoids are unavailable at this time.[14, 15, 16]
Gejala hemorrhoid eksternal yang umumnya dibagi menjadi masalah dengan trombosis akut dan kebersihan / kulit sentuh-sentuhan keluhan. Mantan merespon baik ke kantor eksisi ( tidak enucleation ), sedangkan operasi reseksi reserved untuk yang terakhir. Ingat bahwa terapi ini ditujukan semata-mata di gejala, tidak sama estetika. Bila dilakukan baik, operasi hemorrhoidectomy harus 2-5 % kambuh tingkat. Teknik nonoperative, seperti karet band ligation, menghasilkan kambuh tingkat 30-50 % dalam 5-10 tahun. Namun, rekurensi ini biasanya dapat ditangani dengan pengobatannya nonoperative lebih lanjut Hasil dari 13 jangka panjang prosedur untuk prolapsing wasir tidak tersedia saat ini
Controversies
The major controversies regarding the treatment of hemorrhoids center on the indications for treatment and the choice of operative versus nonoperative therapy. Most experienced surgeons are using office-based nonoperative therapies and are relying less on operative hemorrhoidectomy than they previously were. In the United States, rubber band ligation (compared with injection sclerotherapy) is the mainstay of conservative treatment. Procedure for prolapsing hemorrhoids (PPH), which has been gaining increasing favor in the United States, provides an excellent alternative to operative hemorrhoidectomy for patients with minimal external disease and large internal hemorrhoids.
Kontroversi terbesar tentang pengobatan wasir pusat di indikasi untuk pengobatan dan pilihan operasi versus non-operatif terapi. Ahli bedah yang paling berpengalaman menggunakan terapi non-operatif berbasis kantor dan bergantung kurang pada metode operasi dari mereka sebelumnya. Di Amerika Serikat, karet gelang ligasi (dibandingkan dengan suntikan skleroterapi) adalah andalan pengobatan konservatif. Prosedur untuk dalam wasir (PPH), yang telah mendapatkan semakin menguntungkan di Amerika Serikat, menyediakan alternatif yang sangat baik untuk metode operasi untuk pasien dengan penyakit eksternal yang minimal dan wasir internal yang besar.
Emergency Department Care
Acutely thrombosed external hemorrhoids may be safely excised in the emergency department in patients who present within 48-72 hours of symptom onset. (See Thrombosed External Hemorrhoid Excision)
Infiltration of a local anesthetic containing epinephrine is followed by elliptical incision and excision of the thrombosed hemorrhoid, its accompanying vein, and overlying skin. Simple incision and clot evacuation is inadequate therapy and should not be performed.

Simple incision and clot evacuation is inadequate therapy and should not be performed.
The incision should not extend beyond the anal verge or deeper than the cutaneous layer. A pressure dressing is applied for several hours, after which time the wound is left to heal by secondary intention.
In patients presenting after 72 hours from the start of symptoms, conservative medical therapy is preferable. (See Conservative Management.)
Akut thrombosed eksternal wasir mungkin aman dipotong di gawat darurat pada pasien yang hadir dalam 48-72 jam gejala awal. ( lihat thrombosed hemorrhoid eksternal menghilangkan ) infiltrasi anestesi lokal mengandung epinefrin adalah diikuti oleh elips sayatan dan eksisi thrombosed hemorrhoid, pembuluh darah, yang menyertainya dan overlying kulit. Sayatan sederhana dan clot evakuasi tidak memadai terapi dan tidak harus dilakukan. Sayatan sederhana dan clot evakuasi tidak memadai terapi dan tidak harus dilakukan. Sayatan tidak boleh melampaui anal verge atau lebih dalam dari kulit lapisan. Tekanan yang berpakaian diterapkan selama beberapa jam, setelah itu waktu luka yang tersisa untuk menyembuhkan dengan niat. sekunder Pada pasien menyajikan setelah 72 jam dari awal gejala, konservatif terapi medis adalah lebih baik
Conservative Management
Medical management is the initial treatment of choice for grade I internal and nonthrombosed external hemorrhoids. It consists of warm baths (twice or thrice daily [bid/tid]); a high-fiber diet[17] ; adequate fluid intake; stool softeners; topical and systemic analgesics; proper anal hygiene; and in some cases, a short course of topical steroid cream. A 2012 review indicates a potential benefit of phlebotonics in treating hemorrhoids.[18]
Retraining the patient's toilet habit is also a consideration. Decreasing straining and constipation shrinks internal hemorrhoids and decreases their symptoms; therefore, first-line treatment of all first- and second-degree (and many third- and fourth-degree) internal hemorrhoids should include measures to decrease straining and constipation.
Many patients see improvement or complete resolution of their symptoms with conservative measures. Aggressive therapy is reserved for patients who have persistent symptoms after 1 month of conservative therapy. Treatment is directed solely at symptoms and not at the appearance of the hemorrhoids.
Manajemen medis adalah pengobatan pilihan untuk kelas awal saya internal dan nonthrombosed wasir eksternal. Terdiri dari pemandian air hangat (dua kali atau tiga kali sehari-hari [tawaran/tid]); diet tinggi serat [17]; asupan cairan; bangku pelunak; topikal dan sistemik analgesik; kebersihan anal; dan dalam beberapa kasus, kursus singkat topikal krim steroid. 2012 Review menunjukkan manfaat potensial dari phlebotonics dalam mengobati wasir.[18] Pelatihan ulang pasien toilet kebiasaan ini juga menjadi pertimbangan. Penurunan melelahkan dan sembelit menyusut internal wasir dan mengurangi gejala mereka; oleh karena itu, internal wasir pengobatan lini pertama semua pertama - dan kedua - degree (dan banyak ketiga dan keempat-derajat) harus mencakup langkah-langkah untuk mengurangi melelahkan dan sembelit. Banyak pasien melihat perbaikan atau resolusi lengkap gejala mereka dengan langkah-langkah yang konservatif. Terapi agresif disediakan untuk pasien yang gigih gejala

setelah 1 bulan terapi konservatif. Pengobatan ditujukan semata-mata pada gejala dan bukan pada tampilan wasir.
Warm baths
Bathing in tubs with warm water universally eases painful perianal conditions. Relaxation of the sphincter mechanism and spasm is probably the etiology. Ice can relieve the pain of acute thrombosis.
Some authors do not suggest mechanisms such as the sitz bath for symptom relief. The rigid structure of these portable bathing apparatuses can act in a similar fashion as a toilet seat, causing venous congestion in the perianal area and potentially exacerbating the problem. However, sitz baths do have a role in the treatment of older or immobile patients who cannot routinely get in and out of a bathtub.
Mandi di bak dengan air hangat Universal memudahkan kondisi menyakitkan perianal. Relaksasi sfingter mekanisme dan kejang mungkin adalah etiologi. Es dapat meringankan rasa sakit akut trombosis. Beberapa penulis tidak menyarankan mekanisme seperti sitz mandi untuk meredakan gejala. Struktur kaku aparatur mandi portabel ini dapat bertindak dengan cara yang sama sebagai toilet duduk, menyebabkan vena kemacetan di daerah perianal dan berpotensi memperburuk masalah. Namun, sitz mandi memiliki peran dalam pengobatan pasien remaja atau bergerak yang tidak secara rutin masuk dan keluar dari bak mandi
High-fiber diet
Psyllium seed significantly decreases bleeding and pain compared with placebo. Psyllium seed (Metamucil) and methylcellulose (Citrucel) are the most commonly used supplements. The average American diet consists of 8-15 g of fiber per day; a high-fiber diet includes more than 25 g of fiber per day. Many hemorrhoidal symptoms resolve only when they are treated with dietary alterations, including increased fiber and the addition of fiber supplements.
Psyllium benih secara signifikan menurunkan pendarahan dan rasa sakit dibandingkan dengan plasebo. Psyllium benih ( metamucil ) dan methylcellulose ( citrucel ) adalah yang paling umum digunakan suplemen. Rata-rata orang amerika diet terdiri dari 8-15 g serat per hari; high-fiber diet termasuk lebih dari 25 g serat per hari. Banyak hemorrhoidal gejala menyelesaikan hanya ketika mereka diperlakukan dengan perubahan, makanan termasuk peningkatan serat dan penambahan serat makanan pelengkap.
Antidiarrheal agents, toilet habit retraining, and stool softeners
Antidiarrheal agents are sometimes required in patients with hemorrhoidal symptoms and loose stools. Toilet retraining involves reminding patients that the lavatory is not the library. Patients should sit on the toilet only long enough to evacuate the lower intestines. Persistent straining or prolonged sitting can lead to engorged hemorrhoids.
Agen antidiarrheal kadang-kadang diperlukan pada pasien dengan hemorrhoidal gejala dan longgar bangku. Toilet penopang melibatkan mengingatkan pasien yang toilet tidak perpustakaan. Pasien harus duduk di toilet hanya cukup lama untuk mengevakuasi usus yang lebih rendah. Persistent tegang atau berkepanjangan duduk dapat menyebabkan wasir membesar.

Stool softeners play a limited role in the treatment of routine hemorrhoidal symptoms. Oral fiber intake and fiber supplements almost always cure constipation and straining. Remember that hemorrhoidal symptoms are due to prolapse, thrombosis, and vascular bleeding; therefore, creams and salves have a small role in treating hemorrhoidal complaints. Suppositories, except for providing lubrication, also have a small role in the treatment of hemorrhoidal symptoms.
Bangku softeners memainkan peran yang terbatas dalam pengobatan rutin hemorrhoidal gejala. Asupan serat oral dan serat makanan pelengkap hampir selalu menyembuhkan sembelit dan tegang. Ingat bahwa hemorrhoidal gejala karena prolapse, trombosis, dan pembuluh darah yang berdarah, oleh sebab itu krim dan salves memiliki peran kecil dalam mengobati hemorrhoidal keluhan. Supositoria, kecuali untuk menyediakan pelumasan, juga memiliki peran kecil dalam pengobatan hemorrhoidal gejala
Pelunak feses memiliki peran terbatas dalam mengobati gejala hemoroid. Asupan serat oral dan serat makanan pelengkap dapat menyembuhkan sembelit. Yang perlu diingat bahwa gejala hemoroid dikarenakan adanya prolaps, trombosis, dan pembuluh darah yang mengalami perdarahan, oleh sebab itu krim dan salep memiliki peran kecil dalam mengobati keluhan hemoroid.
Penggunaan steroid topikal belum diteliti dengan baik dalam pengobatan hemoroid, namun agen ini dapat digunakan untuk mengurangi gejala gatal dan peradangan. Topikal hidrokortison kadang-kadang dapat meringankan pendarahan internal. Hal ini penting untuk mempertimbangkan prinsip penggunaan steroid dan efek samping yang terkait, seperti atrofi mukosa. Dengan demikian, penggunaan yang berkepanjangan dari steroid topikal harus dihindari. Beberapa penulis jarang merekomendasikan obat-obatan khas (misalnya, supositoria, krim, enema, busa) dalam pengobatan wasir.
Nitrogliserin topikal dan nifedipin juga telah digunakan untuk meringankan gejala yang berhubungan dengan kejang sfingter anus.[19, 20] obat ini digunakan dengan hati-hati karena efek samping yang terkait, seperti hipotensi. Bukti lain menunjukkan bahwa Diet tinggi serat dapat membantu mengurangi perburukan gejala.
Tersedia berbagai metode non-operatif untuk menghancurkan hemoroid interna. Teknik-teknik non bedah tersebut antara lain dengan karet gelang ligasi, ablasi, sclerosis, atau nekrosis jaringan mukosa.[21, 22, 23]. Teknik tersebut memiliki keuntungan dan kerugian masing-masing. Namun, Semua lini pengobatan pertama dan hemoroid interna derajat dua tidak memerlukan terapi bedah. Semua perawatan non-operatif memiliki keberhasilan yang sama apabila ditangani oleh dokter yang berpengalaman.
Topical agents
The use of topical steroids has not been well-studied in the treatment of thrombosed hemorrhoids; however, these agents can be used to decrease symptoms of pruritus and inflammation. Topical hydrocortisone can sometimes ease internal hemorrhoidal bleeding. It is important to consider the principles of steroid use and the associated side effects, such as mucosal atrophy. As such, the prolonged use of topical steroids should be avoided.

Some authors rarely recommend typical medications (eg, suppository, cream, enema, foam) in the treatment of hemorrhoids. Submucosal veins do not get smaller with anti-inflammatory medications.
Penggunaan steroid topikal belum diteliti dengan baik dalam pengobatan wasir thrombosed; Namun, agen ini dapat digunakan untuk mengurangi gejala gatal dan peradangan. Topikal hidrokortison kadang-kadang dapat meringankan pendarahan dalam internal. Hal ini penting untuk mempertimbangkan prinsip-prinsip penggunaan steroid dan efek samping yang terkait, seperti atrofi mukosa. Dengan demikian, penggunaan yang berkepanjangan dari steroid topikal harus dihindari. Beberapa penulis jarang merekomendasikan obat-obatan khas (misalnya, supositoria, krim, enema, busa) dalam pengobatan wasir. Submukosa vena tidak mendapatkan lebih kecil dengan obat anti-inflamasi.
Topical nitroglycerine and nifedipine have also been used to relieve symptoms associated with anal sphincter spasm.[19, 20] These agents should also be used with caution because of associated side effects, such as hypotension. Good evidence suggests that high-fiber diets in particular help reduce severity and duration of symptoms.
Nitrogliserin topikal dan nifedipin juga telah digunakan untuk meringankan gejala yang berhubungan dengan kejang sfingter dubur.[19, 20] Agen ini juga dapat digunakan dengan hati-hati karena efek samping yang terkait, seperti hipotensi. Baik bukti menunjukkan bahwa Diet tinggi serat khususnya membantu mengurangi keparahan dan durasi gejala.
Nonsurgical Procedures
Numerous nonoperative methods to destroy internal hemorrhoids are available. Nonsurgical techniques function by rubber band ligation, ablation, sclerosis, or necrosis of mucosal tissues.[21, 22, 23] Despite several meta-analyses and considerable personal preference, there is no clear advantage of one technique over the others; however, all should be the first-line treatment of all first- and second-degree internal hemorrhoids that do not respond to conservative therapy. All nonoperative treatments have approximately similar efficacy when administered by an experienced clinician.
Tersedia berbagai metode non-operatif untuk menghancurkan hemoroid interna. Teknik-teknik non bedah tersebut antara lain dengan karet gelang ligasi, ablasi, sclerosis, atau nekrosis jaringan mukosa.[21, 22, 23]. Teknik tersebut memiliki keuntungan dan kerugian masing-masing. Namun, Semua lini pengobatan pertama dan hemoroid interna derajat dua tidak memerlukan terapi bedah. Semua perawatan non-operatif memiliki keberhasilan yang sama apabila ditangani oleh dokter yang berpengalaman.
Lord dilatation, in which the anal canal is manually stretched under anesthesia, is seldom used in the United States, and many colorectal surgeons condemn its use, because it is essentially an uncontrolled disruption of the sphincter mechanism.
Dilatasi, tuhan di mana kanal anal adalah secara manual membentang di bawah anestesi yang, adalah jarang digunakan di amerika serikat, dan banyak ahli bedah kolorektal mengutuk penggunaannya, karena itu yang pada dasarnya sebuah gangguan tidak terkendali sfingter mekanisme
Contraindications for nonsurgical techniques

The following conditions are contraindications for performing the nonsurgical procedures mentioned above:
Acquired immunodeficiency syndrome (AIDS): Human immunodeficiency virus (HIV) infection and anal disease often occur together—conservative therapy is suggested, especially if immunosuppression is evident; poor healing occurs with low CD4 counts, especially when less than 200 cells/mm3
Immunodeficiency disorders Coagulopathy Irritable bowel disease Pregnancy: This condition is associated with many anorectal complaints; nonoperative
treatment or office thrombectomy usually relieves complaints, although operative hemorrhoidectomy is safe in pregnant women[24]
Immediate postpartum period Rectal wall prolapse Large anorectal fissure or infection Tumor
Kondisi berikut apakah contraindications untuk melaksanakan prosedur nonsurgical disebutkan di atas: � acquired immunodeficiency syndrome ( aids ): virus human immunodeficiency ( hiv ) infeksi dan penyakit anal sering terjadi bersama-sama � terapi konservatif adalah menyarankan, terutama jika imunosupresi adalah jelas; miskin penyembuhan terjadi dengan jumlah cd4 rendah menghitung, terutama ketika kurang dari 200 / sel-sel mm3 � gangguan immunodeficiency � coagulopathy � penyakit iritasi usus besar kehamilan �: kondisi ini adalah terkait dengan banyak anorectal keluhan; nonoperative pengobatan atau kantor thrombectomy biasanya mengurangi keluhan, meskipun operatif hemorrhoidectomy adalah aman di wanita hamil 24 � segera periode postpartum � dinding dubur prolapse � anorectal besar fisura atau infeksi � tumor
Rubber band ligation
Rubber band ligation is the most-used remedy for grade II and grade III hemorrhoids and is the standard by which other methods are compared. This procedure is most common in the United States, because it is the most commonly taught method in training programs.[13] With experience, many third-degree and some fourth-degree internal hemorrhoids can be treated nonoperatively.
Blaisdell[25] and Barron[26] described and refined ligation therapy. A band ligature is passed through an anoscope and placed on the rectal mucosa proximal to the dentate line. The tissue necroses and sloughs off in 1-2 weeks, leaving an ulcer that later fibroses. No anesthesia is required; complications are uncommon and usually benign.
When Jutabha et al compared endoscopic rubber band ligation with bipolar electrocoagulation for chronically bleeding grade II or III internal hemorrhoids that were unresponsive to medical therapy, ligation controlled rectal bleeding and other symptoms with significantly fewer treatments (2.3 ± 0.2) and had a significantly higher success rate (92%) than electrocoagulation (3.8 ± 0.4 and 62%, respectively).[27] However, severe pain during treatment occurred more often with ligation (8%) than with electrocoagulation (0%), albeit treatment failure and crossovers were significantly less frequent (8% vs 38%).

Necrotizing pelvic sepsis is a rare, but serious, complication of rubber band ligation. The diagnosis is suggested by the triad of severe pain, fever, and urinary retention. It occurs 1-2 weeks after ligation, frequently in immune-compromised patients, and requires prompt surgical debridement.
Coagulation, electrocautery, and electrotherapy
Infrared coagulation serves best for grades I and II and some grade III hemorrhoids. This method may be as effective as banding with fewer and less severe complications.
Bipolar electrocautery is best for lower-grade hemorrhoids; this technique quickly coagulates the hemorrhoid tissue but has no effect on prolapse.
Low-voltage direct current works best for higher-grade hemorrhoids. Low-voltage direct current requires grounding time and provides excellent control of pain.
Sclerotherapy and cryotherapy
Sclerotherapy can provide adequate treatment of early internal hemorrhoids.[28, 29] However, sclerotherapy and cryotherapy are infrequently used and generally reserved for grade I or II hemorrhoids. Although minimally invasive, these treatment methods have a higher rate of postprocedure pain. Impotence, urinary retention, and abscess formation have also been reported. Recurrence rates are as high as 30%.
Laser therapy and radiowave ablation
Laser therapy is more costly and provides no advantage over other methods. Operators must control the laser to avoid bleeding.
Radiowave ablation followed by suture ligation could prove to be a safe, cost-effective, and convenient way to treat prolapsing hemorrhoids.[30]
Surgical Intervention
Many patients have been referred for surgery because they have severely swollen prolapsed hemorrhoids or very large external skin tags. When questioned, the patients are asymptomatic. Treat hemorrhoids only if they cause problems for the patient. Similarly, patients often ask when they should have surgery. Remind them that their hemorrhoids do not bother anyone else, and they should opt for aggressive treatment only when symptoms become bothersome.
Treatment guidelines are available from the American Gastroenterological Association (AGA)[31] and the American Society of Colon and Rectal Surgeons (ASCRS).[32]
Patients with ulcerative colitis can tolerate aggressive surgery if it is needed. Treat underlying acute disease before any elective anorectal surgery. Avoid aggressive treatment in patients with Crohn disease, especially if the rectal mucosa is acutely inflamed. Drain abscesses as soon as possible, despite active disease elsewhere. If necessary, operative hemorrhoidectomy is safe in pregnant women.[24]

Hemorrhoid surgery can usually be performed using local anesthesia with intravenous (IV) sedation. Regional or general anesthetic techniques also are used. Routine preoperative workup for these techniques is required. Simple distal rectal evacuation is required for a clean operative field. Distal rectal evacuation is best achieved by small-volume saline enemas.
Excision of thromboses
External hemorrhoids generally elicit symptoms due to acute thromboses, recurrent thromboses, or hygiene problems. Manage acute thromboses and recurrent thromboses in a similar fashion. Identify the offending vascular cluster. In the office or clinical setting, inject local anesthetic, and then perform excision of the overlying skin and underlying veins.
Enucleation of the thrombosis alone can result in recurrence of the hemorrhoid at the same spot; excision of the underlying vein completely prevents this event. Electrocoagulation or topical astringent (Monsel solution) provides hemostasis. Suturing the wound closed is not necessary and may cause more pain. Remember, acute thromboses spontaneously resolve in 10-14 days; therefore, a patient who presents late and has diminishing pain is best left alone. Recurrence occurs up to 50% of the time when thromboses are left alone.
Surgical hemorrhoidectomy
Surgical hemorrhoidectomy is the most effective treatment for all hemorrhoids and in particular is indicated in the following situations:
Conservative or nonsurgical treatment fails (persistent bleeding or chronic symptoms) Grade III and IV hemorrhoids with severe symptoms Presence of concomitant anorectal conditions (eg, anal fissure or fistula, hygiene trouble
caused by large skin tags, a history of multiple external thromboses, or internal hemorrhoid trouble) requiring surgery
Patient preference
About 5-10% of people with hemorrhoids eventually require surgical hemorrhoidectomy. Proper anesthetic care (especially if local anesthesia with supplementary IV sedation), attention to perioperative fluid restriction, and careful postoperative instructions can ease the patient's recovery.
Postoperative pain remains the major complication, with most patients requiring 2-4 weeks before returning to normal activities. Other possible complications include urinary retention, anal stenosis, and incontinence.
Nonlaser versus laser hemorrhoidectomy
Laser hemorrhoidectomy, as opposed to conventional scalpel and electrocautery techniques, is associated with many myths. Hemorrhoidectomy factories have touted painless or decreased pain and shortened healing times as advantages to performing hemorrhoidectomies by laser. No documented studies support these claims. In fact, one prospective study found no difference between scalpel and laser hemorrhoidectomy.[33] The reader is referred to appropriate textbooks to see descriptions of techniques used.[34, 35]
Stapled hemorrhoid surgery/ procedure for prolapsing hemorrhoids (PPH)

Stapled hemorrhoid surgery, or PPH, was first described in 1997-1998 and has become prominent.[36, 37, 14] This procedure is mainly used to treat internal hemorrhoids that are not amenable to conservative and nonoperative therapies. PPH is suggested for patients with large internal hemorrhoids and minimal external component. This procedure can be done in an outpatient setting with local anesthesia,[38, 39, 40, 41] similar to the protocol used for conventional hemorrhoid surgery. Narcotic use and recovery is significantly decreased compared with conventional operative hemorrhoid surgery.
During this procedure, a specially designed circular stapler with smaller staples is used. The technique involves placing a suture in the mucosal and submucosal layers circumferentially, approximately 3-4 cm above the dentate line. The stapler is placed and slowly closed around the purse string. Care is taken to draw excess internal hemorrhoidal tissue into the stapler. The stapler is fired, resecting the excess tissue and placing a circular staple line above the dentate line, resulting in resection of excessive internal hemorrhoidal tissue, pexy of the internal hemorrhoidal tissue left behind, and interruption of the blood supply from above.
PPH does not directly affect the external tissue. Reports have described shrinking of external hemorrhoidal tissue after PPH, probably from decreased blood flow. Good results from PPH combined with judicial excision of occasional skin tags also have been reported.
Acute hemorrhoidal crisis
Acute hemorrhoidal crisis is a rare event that usually requires emergency treatment. The mechanism of action is a large internal hemorrhoid prolapse. The sphincter mechanism squeezes, incarcerating the internal hemorrhoids and strangulating them. The resulting spasm causes edema and occasionally thrombosis of the external hemorrhoids. The resulting pain and swelling are dramatic and very painful. Emergent operative resection is safe and, with conservation of the anoderm, provides good relief. Rapid pain relief with office excision of thromboses and ligation of internal hemorrhoids has been reported.
Long-Term Monitoring
After excision of a thrombosed external hemorrhoid, the patient may be discharged home for several hours of bedrest followed by warm baths 2-3 times daily, stool softeners, and topical or systemic analgesia. The patient should return in 48-72 hours for a wound check.
All other patients should be referred to a surgical or rectal clinic for more definitive treatment and sent home with conservative medical therapy.
Monitor patients at regular intervals until they are healed and have no symptoms.
Attention to regular and soft bowel movements is important. Bulk agents (eg, psyllium seed) and oral fluids are important. Bathing in tubs for comfort and hygiene is part of the routine. Judicious narcotic administration relieves pain.[42] Patients should also be advised of the following:
Avoid constipation Weight loss Avoid prolonged sitting on the toilet Avoid prolonged sitting at work

Improved anorectal hygiene
REFERENCES
1. Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen's Emergency Medicine: Concepts and Clinical Practice. 6th ed. Philadelphia, Pa: Elsevier; 2006:1509-12.
2. Tintinalli JE, Kelen GD, Stapczynski JS, eds. Emergency Medicine: A Comprehensive Study Guide. 6th ed. New York, NY: McGraw Hill; 2004:540-1.
3. Ibrahim AM, Hackford AW, Lee YM, Cave DR. Hemorrhoids can be a source of obscure gastrointestinal bleeding that requires transfusion: report of five patients. Dis Colon Rectum. Aug 2008;51(8):1292-4. [Medline].
4. Grucela A, Salinas H, Khaitov S, Steinhagen RM, Gorfine SR, Chessin DB. Prospective analysis of clinician accuracy in the diagnosis of benign anal pathology: comparison across specialties and years of experience. Dis Colon Rectum. Jan 2010;53(1):47-52. [Medline].
5. Gibbons CP, Bannister JJ, Read NW. Role of constipation and anal hypertonia in the pathogenesis of haemorrhoids. Br J Surg. Jul 1988;75(7):656-60. [Medline].
6. Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology. Feb 1990;98(2):380-6. [Medline].
7. Johanson JF, Sonnenberg A. Constipation is not a risk factor for hemorrhoids: a case-control study of potential etiological agents. Am J Gastroenterol. Nov 1994;89(11):1981-6. [Medline].
8. Bernstein WC. What are hemorrhoids and what is their relationship to the portal venous system?. Dis Colon Rectum. Dec 1983;26(12):829-34. [Medline].
9. Hosking SW, Smart HL, Johnson AG, Triger DR. Anorectal varices, haemorrhoids, and portal hypertension. Lancet. Feb 18 1989;1(8634):349-52. [Medline].
10. Johansen K, Bardin J, Orloff MJ. Massive bleeding from hemorrhoidal varices in portal hypertension. JAMA. Nov 7 1980;244(18):2084-5. [Medline].
11. Chawla Y, Dilawari JB. Anorectal varices--their frequency in cirrhotic and non-cirrhotic portal hypertension. Gut. Mar 1991;32(3):309-11. [Medline]. [Full Text].
12. Katz JA, Rubin RA, Cope C, Holland G, Brass CA. Recurrent bleeding from anorectal varices: successful treatment with a transjugular intrahepatic portosystemic shunt. Am J Gastroenterol. Jul 1993;88(7):1104-7. [Medline].
13. El Nakeeb AM, Fikry AA, Omar WH, Fouda EM, El Metwally TA, Ghazy HE, et al. Rubber band ligation for 750 cases of symptomatic hemorrhoids out of 2200 cases. World J Gastroenterol. Nov 14 2008;14(42):6525-30. [Medline]. [Full Text].
14. Raahave D, Jepsen LV, Pedersen IK. Primary and repeated stapled hemorrhoidopexy for prolapsing hemorrhoids: follow-up to five years. Dis Colon Rectum. Mar 2008;51(3):334-41. [Medline].
15. Jayaraman S, Colquhoun PH, Malthaner RA. Stapled hemorrhoidopexy is associated with a higher long-term recurrence rate of internal hemorrhoids compared with conventional excisional hemorrhoid surgery. Dis Colon Rectum. Sep 2007;50(9):1297-305. [Medline].

16. Ceci F, Picchio M, Palimento D, Calì B, Corelli S, Spaziani E. Long-term outcome of stapled hemorrhoidopexy for Grade III and Grade IV hemorrhoids. Dis Colon Rectum. Jul 2008;51(7):1107-12. [Medline].
17. Moesgaard F, Nielsen ML, Hansen JB, Knudsen JT. High-fiber diet reduces bleeding and pain in patients with hemorrhoids: a double-blind trial of Vi-Siblin. Dis Colon Rectum. Jul-Aug 1982;25(5):454-6. [Medline].
18. Perera N, Liolitsa D, Iype S, Croxford A, Yassin M, Lang P, et al. Phlebotonics for haemorrhoids. Cochrane Database Syst Rev. Aug 15 2012;8:CD004322. [Medline].
19. Gorfine SR. Treatment of benign anal disease with topical nitroglycerin. Dis Colon Rectum. May 1995;38(5):453-6; discussion 456-7. [Medline].
20. Perrotti P, Antropoli C, Molino D, De Stefano G, Antropoli M. Conservative treatment of acute thrombosed external hemorrhoids with topical nifedipine. Dis Colon Rectum. Mar 2001;44(3):405-9. [Medline].
21. Yuksel BC, Armagan H, Berkem H, Yildiz Y, Ozel H, Hengirmen S. Conservative management of hemorrhoids: a comparison of venotonic flavonoid micronized purified flavonoid fraction (MPFF) and sclerotherapy. Surg Today. 2008;38(2):123-9. [Medline].
22. Faucheron JL, Gangner Y. Doppler-guided hemorrhoidal artery ligation for the treatment of symptomatic hemorrhoids: early and three-year follow-up results in 100 consecutive patients. Dis Colon Rectum. Jun 2008;51(6):945-9. [Medline].
23. Johanson JF, Rimm A. Optimal nonsurgical treatment of hemorrhoids: a comparative analysis of infrared coagulation, rubber band ligation, and injection sclerotherapy. Am J Gastroenterol. Nov 1992;87(11):1600-6. [Medline].
24. Saleeby RG Jr, Rosen L, Stasik JJ, Riether RD, Sheets J, Khubchandani IT. Hemorrhoidectomy during pregnancy: risk or relief?. Dis Colon Rectum. Mar 1991;34(3):260-1. [Medline].
25. BLAISDELL PC. Prevention of massive hemorrhage secondary to hemorrhoidectomy. Surg Gynecol Obstet. Apr 1958;106(4):485-8. [Medline].
26. BARRON J. Office ligation treatment of hemorrhoids. Dis Colon Rectum. Mar-Apr 1963;6:109-13. [Medline].
27. Jutabha R, Jensen DM, Chavalitdhamrong D. Randomized prospective study of endoscopic rubber band ligation compared with bipolar coagulation for chronically bleeding internal hemorrhoids. Am J Gastroenterol. Aug 2009;104(8):2057-64. [Medline].
28. Senapati A, Nicholls RJ. A randomised trial to compare the results of injection sclerotherapy with a bulk laxative alone in the treatment of bleeding haemorrhoids. Int J Colorectal Dis. Jun 1988;3(2):124-6. [Medline].
29. Thornton SC. Sclerotherapy of hemorrhoids. Selected Topics in Colon and Rectal Surgery. Vol 5. Norwalk, Conn: Konsyl Pharmaceuticals; 1992:72-5..
30. Gupta PJ, Kalaskar S. Radiowave ablation and mucopexy for prolapsing hemorrhoids--a pilot study. Int J Surg. Jun 2009;7(3):223-7. [Medline].
31. American Gastroenterological Association medical position statement: Diagnosis and treatment of hemorrhoids. Gastroenterology. May 2004;126(5):1461-2. [Medline].
32. Cataldo P, Ellis CN, Gregorcyk S, Hyman N, Buie WD, Church J, et al. Practice parameters for the management of hemorrhoids (revised). Dis Colon Rectum. Feb 2005;48(2):189-94. [Medline].
33. Leff EI. Hemorrhoidectomy--laser vs. nonlaser: outpatient surgical experience. Dis Colon Rectum. Aug 1992;35(8):743-6. [Medline].

34. Corman M. Hemorrhoid. In: Corman M. Colon and Rectal Surgery. Philadelphia, Pa: Lippincott-Raven; 1998:154-6.
35. Mazier WP. Hemorrhoids: surgery of the colon. In: Maxier WP, Levm DH, Luchtefeld. MA, Senagore AJ, eds. Rectum and Anus. Philadelphia, Pa: WB Saunders; 1995:229-54.
36. Esser S, Khubchandani I, Rakhmanine M. Stapled hemorrhoidectomy with local anesthesia can be performed safely and cost-efficiently. Dis Colon Rectum. Jul 2004;47(7):1164-9. [Medline].
37. Ho YH, Cheong WK, Tsang C, Ho J, Eu KW, Tang CL, et al. Stapled hemorrhoidectomy--cost and effectiveness. Randomized, controlled trial including incontinence scoring, anorectal manometry, and endoanal ultrasound assessments at up to three months. Dis Colon Rectum. Dec 2000;43(12):1666-75. [Medline].
38. Senagore AJ, Singer M, Abcarian H, Fleshman J, Corman M, Wexner S, et al. A prospective, randomized, controlled multicenter trial comparing stapled hemorrhoidopexy and Ferguson hemorrhoidectomy: perioperative and one-year results. Dis Colon Rectum. Nov 2004;47(11):1824-36. [Medline].
39. Behboo R, Zanella S, Ruffolo C, Vafai M, Marino F, Scarpa M. Stapled haemorrhoidopexy: extent of tissue excision and clinical implications in the early postoperative period. Colorectal Dis. Jun 2011;13(6):697-702. [Medline].
40. Pattana-arun J, Wesarachawit W, Tantiphlachiva K, Atithansakul P, Sahakitrungruang C, Rojanasakul A. A comparison of early postoperative results between urgent closed hemorrhoidectomy for prolapsed thrombosed hemorrhoids and elective closed hemorrhoidectomy. J Med Assoc Thai. Dec 2009;92(12):1610-5. [Medline].
41. Bove A, Bongarzoni G, Palone G, Chiarini S, Calisesi EM, Corbellini L. Effective treatment of haemorrhoids: early complication and late results after 150 consecutive stapled haemorrhoidectomies. Ann Ital Chir. Jul-Aug 2009;80(4):299-303. [Medline].
42. Perrotti P, Dominici P, Grossi E, Cerutti R, Antropo li C. Topical nifedipine with lidocaine ointment versus active control for pain after hemorrhoidectomy: results of a multicentre, prospective, randomized, double-blind study. Can J Surg. Feb 2010;53(1):17-24. [Medline]. [Full Text].
43. Halverson A. Hemorrhoids. Clin Colon Rectal Surg. May 2007;20(2):77-85. [Medline]. [Full Text].
44. Koning MV, Loffeld RJ. Rectal bleeding in patients with haemorrhoids. Coincidental findings in colon and rectum. Fam Pract. Jun 2010;27(3):260-2. [Medline].

BAB 2
TINJAUAN PUSTAKA

Anatomi Kanalis Anal
Kanalis anal memiliki panjang sekitar 4 cm, yang dikelilingi dengan mekanisme sfingter anus. Setengah bagian atas dari kanalis anal dilapisi oleh mukosa glandular rektal. Mukosa bagian teratas dari kanalis anal berkembang sampai 6-10 lipatan longitudinal, yang disebut columns of Morgagni, yang masing masing memiliki cabang terminal dari arteri rektal superior dan vena. Lipatan -lipatan ini paling menonjol di bagian lateral kiri, posterior kanan dan kuadran anterior kanan, dimana vena membentuk pleksus vena yang menonjol. Mukosa glandular relatif tidak sensitif, berbeda dengan kulit kanalis, kulit terbawahnya lebih sensitif .
Mekanisme spinter anal memiliki tiga unsur pembentuk, spinter internal, spinter eksternal dan puborektalis. Spinter internal merupakan kontinuasi yang semakin menebal dari muskular dinding ginjal. Spinter eksternal dan puborektalis sling (yang merupakan bagian dari levator ani) muncul dari dasar pelvis. Vaskularisasi rektum dan kanalis anal sebagian besar diperoleh melalui arteri hemoroidalis superior, media, dan inferior. Arteri hemoroidalis superior merupakan kelanjutan akhir arteri mesentrika inferior. Arteri hemoroidalis media merupakan cabang ke anterior dari arteri hipogastrika. Arteri hemoroidalis inferior dicabangkan oleh arteri pubenda interna yang merupakan cabang dari arteri iliaca interna, ketika arteri tersebut melewati bagian atas spina ischiadica. Sedangkan vena -vena dari kanalis anal dan rektum mengikuti perjalanan yang sesuai dengan perjalanan arteri. Vena -vena ini berasal dari 2 pleksus yaitu pleksus hemoroidalis superior (interna) yang terletak di submukosa atas anorectal junction dan pleksus hemoroidalis inferior (eksterna) yang terletak dibawah anorectal junction dan di luar lapisan otot.
Vaskularisasi Vena -Vena Kanalis Anal
Persarafan rektum terdiri atas sistem saraf simpatik dan parsimpatik. Serabut saraf simpatik berasal dari pleksus mesentrikus inferior dan dari sistem parasakral yang terbentuk dari ganglion simpatis lumbal ruas kedua, ketiga, dan keempat. Persarafan parasimpatik (nervi erigentes) berasal dari saraf sakral kedua, ketiga, dan keempat.
Fisiologi Rektum dan Anus
Fungsi utama dari rektum dan kanalis anal ialah untuk mengeluarkan massa feses yang terbentuk di tempat yang lebih tinggi dan melakukan hal tersebut dengan cara yang terkontrol. Rektum dan kanalis anal tidak begitu berperan dalam proses pencernaan, selain hanya menyerap sedikit cairan. Selain itu sel-sel Goblet mukosa mengeluarkan mukus yang berfungsi sebagai pelicin untuk keluarnya massa feses.
Pada hampir setiap waktu rektum tidak berisi feses. Hal ini sebagian diakibatkan adanya otot sfingter yang tidak begitu kuat yang terdapat pada rectosimoid junction, kira -kira 20 cm dari anus. Terdapatnya lekukan tajam dari tempat ini juga memberi tambahan penghalang masuknya feses ke rektum. Akan tetapi, bila suatu gerakan usus mendorong feses ke arah rektum, secara normal hasrat defekasi akan timbul, yang ditimbulkan oleh refleks kontraksi dari rektum dan relaksasi dari otot sfingter. Feses tidak keluar secara terus-menerus dan sedikit demi sedikit dari anus berkat adanya kontraksi tonik otot sfingter ani interna dan eksterna .
Definisi Hemoroid

Hemoroid adalah kumpulan dari pelebaran satu segmen atau lebih vena
hemoroidalis di daerah anorektal. Hemoroid bukan sekedar pelebaran vena
hemoroidalis, tetapi bersifat lebih kompleks yakni melibatkan beberapa uns
ur berupa
pembuluh darah, jaringan lunak dan otot di sekitar anorektal (kanalis anus). Secara
keseluruhan berdasarkan statistic, jumlah tindakan hemoroidektomi menurun.
Puncaknya terjadi tahun 1974 dimana hemoroidektomi dilakukan sebanyak 117 per
100.000 o
rang. Angka itu menurun 13 tahun kemudian (1987) menjadi 37 per
100.000 orang (Felix, 2006).
Hemoroid merupakan dilatasi varises pleksus vena submukosa anus dan
perianus. Dilatasi ini sering terjadi setelah usia 50 tahun yang berkaitan dengan
peningkatan tekanan vena di dalam pleksus hemoroidalis (Robbins, 2007).
Universitas
Sumatera
Utara
2.
4.
Faktor Resiko
Hemoroid memiliki faktor resiko yang cukup banyak antara lain kurangnya
mobilisasi, konstipasi, cara buang air besar yang tidak benar, kurang minum, kurang
memakan makanan berserat
(sayur dan buah), faktor genetika, kehamilan, penyakit
yang meningkatkan tekanan intraabdomen (tumor abdomen, tumor usus), dan sirosis
hati (Simadibrata, 2006).
Konstipasi merupakan etiologi hemoroid yang paling sering. Konstipasi
terjadi apabila feses me
njadi terlalu kering, yang timbul karena defekasi yang

tertunda terlalu lama. Jika isi kolon tertahan dalam waktu lebih lama dari normal,
jumlah H2O yang diserap akan melebihi normal, sehingga feses menjadi kering dan
keras (Sherwood, 2001).
Kejadian hemor
oid
umumnya
sebanding
pada
laki
-
laki maupun perempuan.
Sekitar setengah orang yang berumur 50 tahun pernah mengalami hemoroid.
Hemoroid juga terjadi pada
wanita hamil.
Pada wanita hamil, janin pada uterus,
serta
perubahan hormonal, menyebabkan
pembuluh dar
ah hemoroidalis meregang.
Semua
vena dapat diperparah saat terjadinya tekanan selama persalinan. Hemoroid pada
wanita hamil hanya merupakan komplikasi yang bersifat sementara (
Pearl, 2004).
2.5.
Gejala Klinis
Hemoroid
merupakan salah satu

ke luhan ko lorekt al ya
ng paling umum
dide ngar oleh
dokter. Setiap tahun sekitar 10,5 juta
Amerika mengalami gejala
hemoroid;
seperempat pasien
harus berkonsulta
si
.
Gejala yang paling umum dari
hemoroid
yaitu
darah merah
yang cerah
menutupi toilet duduk
dan
muncul di atas
kertas
toilet.
G
ejala
lain
termasuk iritasi ku lit di sekitar anus
,
rasa sakit, bengkak, atau
benjolan keras di sekitar anus

, dan
didapati
lendir
pada sekitar anus
.
Terlalu banyak
menggosok atau membersihkan sekitar anus dapat memperburuk gejala dan bahkan
menyeb
abkan iritasi yang semakin parah, berdarah, dan gatal
-
gatal yang disebut
pruritus ani
(Parker, 2004).
Universitas
Sumatera
Utara
H
emorhoid sering menimbulkan gejala
-
gejala secara tidak beraturan.
Menurut Churchill (1990) gejala
-
gejala hemoroid adalah :
1.
Iritasi da n benjolan per
ianal, serta gatal
-
gatal ( pruritus ani),

2.
Rasa tidak nyaman di daerah anus dan nyeri yang semakin diperberat oleh
buang air besar (BAB),
3.
Prolapse hemorrhoida lis,
4.
Pendarahan rektal.
2.6.
Klasifikasi dan Derajat Hemoroid
Berdasarkan letaknya, hemoroid dibagi
menjadi 3 yaitu hemoroid eksterna,
interna, dan campuran. Dikatakan eksterna karena benjolan terletak dibawah linea
pectinea. Hemoroid eksterna mempunyai 3 bentuk yaitu bentuk hemoroid biasa yang
letaknya distal linea pectinea, bentuk trombosis, dan bentuk
skin tags
. Biasanya
benjolan pada hemoroid eksterna akan keluar dari anus bila mengedan, tapi dapat
dimasukkan kembali dengan jari. Rasa nyeri pada perabaan menandakan adanya
trombosis, yang biasanya disertai penyulit seperti infeksi atau abses perianal (
Felix,
2006).
Berlawanan dengan hemoroid eksterna, benjolan pada hemoroid interna
terletak diatas linea pectinea. Hemoroid interna merupakan benjolan dari vena
hemoroidalis internus yang dilapisi epitel dari mukosa anus. Pada posisi litotomi,
benjolan paling sering terdapat pada jam 3, 7, dan 11. Ketiga letak itu dikenal dengan
three primary haemorrhoidal areas
(Felix, 2006).

Hemoroid interna dapat prolaps saat mengedan dan kemudian terperangkap
akibat tekanan sfingter anus sehingga terjadi pembesaran menda
dak yang edematosa,
hemoragik, dan sangat nyeri. Kedua klasifikasi hemoroid tersebut memiliki pembuluh
darah yang melebar, berdinding tipis, dan mudah berdarah, kadang
-
kadang menutupi
perdarahan dari lesi proksimal yang lebih serius (Robbins, 2007).
Deraja
t hemoroid interna dibagi berdasarkan gamabaran klinis, yaitu:
Universitas
Sumatera
Utara
1.
D
erajat 1
:
Bila terjadi pembesaran hemoroid yang tidak prolaps ke luar
kanal anus.
Hanya dapat dilihat dengan anorektoskop.
2.
Derajat 2
:
Pembesaran hemoroid yang prolaps dan menghilang atau
masuk sendiri ke dalam anus secara spontan.
3.
Derajat 3
:

Pembesaran hemoroid yang prolaps dapat masuk lagi ke dalam
anus dengan bantuan dorongan jari.
4.
Derajat 4
:
Prolaps hemoroid yang permanen. Rentan dan cenderung untuk
mengalami trombosis dan infark.
Untuk melihat resiko perdarahan hemoroid, dapat dideteksi oleh adanya
stigma perdarahan berupa bekuan darah yang masih menempel, erosi, kemerahan di
atas hemoroid
(Simadibrata
, 2006
).
2.7.
Patofisiologi Hemoroid
Hemoroid dikatakan sebagai penyakit keturunan. N
amun sampai saat ini
belum terbukti kebenarannya. Akhir
-
akhir ini, keterlibatan bantalan anus (anal
cushion) makin dipahami sebagai dasar terjadinya penyakit ini.
Bantalan anus
merupakan jaringan lunak yang kaya akan pembuluh darah. Agar stabil,
kedudukann
ya disokong oleh ligamentum Treitz dan lapisan muskularis submukosa.
Bendungan dan hipertrofi pada bantalan anus menjadi mekanisme dasar terjadinya
hemoroid.

Pertama
, kegagalan pengosongan vena bantalan anus secara cepat saat
defekasi.
Kedua
, bantalan anus
terlalu mobile, dan
ketiga
, bantalan anus terperangkap
oleh sfingter anus yang ketat. Akibatnya, vena intramuskular kanalis anus akan
terjepit (obstruksi). Proses pembendungan diatas diperparah lagi apabila seseorang
mengedan atau adanya feses yang keras
melalui dinding rektum (Felix, 2006).
Selain itu, gangguan rotasi bantalan anus juga menjadi dasar terjadinya
keluhan hemoroid. Dalam keadaan normal, bantalan anus menempel secara longgar
pada lapisan otot sirkuler. Ketika defekasi, sfingter interna akan r
elaksasi. Kemudian,
bantalan anus berotasi ke arah luar (eversi) membentuk bibir anorektum. Faktor
Universitas
Sumatera
Utara
e
ndokrin, usia, konstipasi dan mengedan yang lama menyebabkan gangguan eversi
pada bantalan tersebut. Mitos di masyarakat yang mengatakan, hemoroid mudah
ter
jadi pada ibu hamil ternyata benar. Tak pelak, kehamilan menjadi faktor pencetus
hemoroid. Mengapa demikian?
Pertama
, hormon kehamilan mengurangi fungsi

penyokong dari otot dan ligamentum di sekitar bantalan.
Kedua
, terjadi peningkatan
vaskuler di daerah p
elvis.
Ketiga
, seringnya terjadi konstipasi pada masa kehamilan.
Dan terakhir adalah kerusakan kanalis anus saat melahirkan pervaginam (Felix,
2006).
2.8.
Diagnosa
Diagnosis hemoroid ditegakkan berdasarkan anamnesis keluhan klinis dari
hemoroid berda sarka n kla
sifikasi hemoroid (derajat 1 sampai dengan derajat 4), dan
pemeriksaan anoskopi/kolonoskopi. Karena hemoroid disebabkan adanya tumor
didalam abdomen atau usus proksimal, agar lebih teliti selain memastikan diagnosis
hemoroid, dipastikan juga apakah di usus
halus
atau di kolon ada kelainan mi
sal,
tumor atau colitis.
Untuk memastikan kelainan di usus halus diperlukan pemeriksaan
rontgen usus halus atau enteroskopi. Sedangkan untuk memastikan kelainan di kolon
diperlukan pemeriksaan rontgen Barium enema atau k
olonoskopi total
(Simadibrata
,

2006
).
2.9.
Diagnosa Banding
Banyak masalah anorektal, antara lain, fistula,
abses, atau iritasi dan gatal
-
gatal, yang memiliki
gejala mirip dengan hemoroid dan
harus dipahami sebelum
direkomendasikan untuk melakukan
pengobatan
. Selain itu,
hubungan
pendarahan
anus dengan kanker kolorektal menjadi
kuat
jika dikaitkan dengan
usia
.
Oleh karena
itu, evaluasi lebih
lanjut
dengan kolonoskopi harus dilakukan pada pasien
yang lebih
tua dari 50 tahun
serta keluarga yang memiliki riwayat

kanker usus besar
(Parker,
2004)
Universitas
Sumatera
Utara
2.
10.
Penatalaksanaan Hemoroid
Menangani hemoroid tak perlu terus melakukan tindakan invasif. Dengan obat
juga dapat dilakukan. Namun, pemilihan jenis terapi (obat atau invasif) sangat
bergantung dari keluhan penderita serta der
ajat hemoroidnya. Tidak ada indikasi
mutlak dalam terapi invasif dan diusahakan menjadi pilihan terakhir. Salah satu obat
hemoroid adalah diosmin dan hesperidin yang dimikronisasi. Layaknya
noreadrenalin, obat ini mengakibatkan kontraksi vena, menurunkan e
kstravasasi dari
kapiler dan menghambat reaksi inflamasi terhadap prostaglandin (PGE2, PGF2).
Kehadiran obat ini tentu memberi angin segar bagi penderita hemoroid yang takut
atau
enggan
dioperasi. Sebuah studi acak bahkan membuktikan obat ini sama efektif
dengan
rubber band
ligation
. Malah dengan efek samping lebih kecil. Bila obat sudah
tak adekuat atau terjadi perdarahan dan prolaps, tindakan invasif menjadi pilihan
terakhir. Prinsip dari tindakan invasif ada 2 yaitu fiksasi dan eksisi. Fiksasi dilakukan

pada derajat I dan II.
Dan selebihnya adalah eksisi (Felix, 2006).
Fiksasi
terdiri dari:.
1.
Skleroterapi
. Dilakukan untuk menghentikan perdarahan. Metode ini
menggunakan zat sklerosan yang disuntikan para vasal. Setelah itu, sklerosan
merangsang pembentukan jaringan parut sehingga menghambat aliran darah ke
vena
-
vena hemoroidalis. Akibatnya, perdarahan berhenti. Sklerosan yang dipakai
adalah 5%
phenol in almond oil
dan 1%
polidocanol
.
Metode ini mudah
dilaksanakan, aman dan memberikan hasil baik.
2.
Rubber band
ligation
. Kerja dari metode ini adalah akan mengabliterasi lokal
vena hemoroidalis sampai terjadi ulserasi (7
-
10 hari) yang diikut i terjadinya
jaringan parut (3

-
4 minggu). Prosedur ini dilakukan pada hemoroid derajat
1-3.
3.
Infrared thermocoagulati
on
. Prinsipnya adalah mendenaturasi protein melalui
efek panas dari
infrared
, yang selanjutnya mengakibatkan jaringan terkoagulasi.
Untuk mencegah efek samping dari
infrared
berupa kerusakan jaringan sekitar
Universitas
Sumatera
Utara
y
ang sehat, maka jangka waktu paparan dan kedalamannya perlu diukur akurat.
Metode ini diperuntukkan pada derajat 1
-
2.
4.
Laser haemorrhoidectomy
. Metode ini mirip dengan
infrared
. Hanya saja
mempunyai kelebihan dalam kemampuan memotong. Namun, biayanya mahal.
5.

Doppler ultrasound guided haemorrhoid artery l
igation
.
Metode ini menjadi
pilihan utama saat terjadi perdarahan karena dapat mengetahui secara tepat lokasi
arteri hemoroidalis yang hendak dijahit.
6.
Cryotherapy
. Metode ini kurang direkomendasikan karena seringkali kurang
akurat dalam menentukan area
freezing
.
Sedangkan eksisi
dapat dilakukan dengan beberapa teknik yaitu
St. Marks
Milligan
–
Morgan Technique
,
Submucosal Haemorrhoidectomy
(
Parks method
), dan
yang terbaru adalah
Circular Stapler Anopexy
(teknik Longo). Teknik
Circular

Stapler Anopexy
atau
dikenal dengan
Procedure for Prolapse and Haemorrhoids
(PPH) baru dikembangkan sekitar tahun 1993. Teknik ini bekerja dengan mendorong
jaringan hemoroid yang merosot ke arah atas dan dijahitkan ke selaput lendir dinding
anus. Kemudian sebuah gelang dari ba
han titanium diselipkan di jahitan dan
ditanamkan di bagian atas saluran anus untuk mengokohkan posisi jaringan hemoroid
tersebut. PPH memiliki beberapa keuntungan dibandingka n operasi konvensional
diantaranya, nyeri minimal karena tindakan dilakukan di lu
ar bagian sensitif, tindakan
cepat karena hanya menghabiskan 12
-
45 menit, dan pasien dapat pulih lebih cepat
pasca operasi. Namun risiko perdarahan, trombosis, serta penyempitan saluran anus
masih dapat terjadi. Kontraindikasi PPH adalah fistula anus, beng
kak, gangren,
penyempitan anus, prolaps jaringan hemoroid yang tebal, serta pada pasien dengan
gangguan koagulasi (pembekuan darah) (Felix, 2006).
Komplikasi yang dapat timbul pasca tindakan invasif adalah perdarahan
sekunder, selulitis, abses, fistula, fi
ssura, dan inkontinensia. Hemoroid bukan
penyakit yang tak mungkin dicegah. Dengan mengkonsumsi tinggi serat seperti
Universitas
Sumatera
Utara
b

anyak sayur dan buah akan membuat feses lembek sehingga tidak perlu mengedan
saat buang air besar (Felix, 2006).
Menurut Haryoga (2009), a
da banyak hal yang bisa dilakukan untuk
mencegah berulangnya kekambuhan keluhan hemoroid, di antaranya :
1.
Hindari mengedan terlalu kuat saat buang air besar.
2.
Cegah konstipasi dengan banyak mengonsumsi makanan kaya serat (sayur
dan buah serta kacang
-
kacangan
) serta banyak minum air put ih minimal
delapan gelas sehari untuk melancarkan defekasi.
3.
Jangan menunda
-
nunda jika ingin buang air besar sebelum feses menjadi
keras.
4.
Tidur cukup.
5.
Jangan duduk terlalu lama.
6.
Senam/olahraga rutin.
Universitas
Sumatera
Utara

Related Documents