Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


Menghilangkan stress, baik fisik maupun
psikis akibat tindakan – tindakan medik
terhadap bayi atau anak dengan aman.
Langkah awal untuk mencapai tujuan
tersebut adalah memahami fisiologis dan
anatomi bayi yang sangat berbeda
dengan orang dewasa.

1. Airway (Jalan Nafas)
2.Sistem Pernafasan
3. Sistim kardiovaskuler
4. Kebutuhan cairan-elektrolit-metabolisme
5. Pengaturan suhu tubuh
6. Psikologi

Jalan nafas mudah tersumbat :
1. Kepala relatif besar
2. Leher lebih pendek
3. Lubang hidung (nares) sempit
4. Lidah besar
5. Epiglottis besar, terkulai dan berbentuk U
6. Edema jalan nafas dapat fatal


Expansi paru2 terbatas :
1. Rongga dada sempit
2. CTR anak > dewasa
3. Abdomen besar
4. Diafragma tinggi
5. Posisi iga horisontal
6. Otot intercostal belum sempurna

Dewasa Anak/bayi


Nadi bayi 120-180
Nadi anakumur 4 tahun 100
Nadi anak umur 10 tahun 90
Pada anak bradicardi lebih ditakutkan
daripada takikardi.
Pengamatan tensi lebih penting karena
batasan keamanannya sempit sehingga
mudah jatuh ke dalam keadaan shock
ASUS
Highlight

Mudah bradikardi :
* Nyeri
* Rangsangan jalan nafas - Intubasi
- Suction
* Hipoxia , Hiperkarbia.
* Pemberian obat tertentu
Bradikardi ~ cardiac output yang menurun :
* Stroke volume fixed
* Prevensi/terapi – Sulfas Atropin.

Batas keselamatan sempit * Estimated Blood Volume (perkiraan jumlah darah) bayi 85 ml/kg = 250 ml dewasa 65 ml/kg = 3500 ml * Perdarahan 50 ml sesuai dengan presyok * Mudah overload.(cairan berlebihan). Hemoglobin * 12 – 19 g% * HbF 80% mengakibatkan affinitas ikatan terhadap
Oksigen meningkat * Hematokrit 50%. Kelainan Kongenital JAntung * ASD , Potent Ductus Arteriosus, Tetralogi Fallot.
ASUS
Highlight


Rumatan/Kebutuhan sehari-hari.
* Keringat.
* Eksresi
* Uap pernafasan.
* Pertumbuhan.
Cairan Pengganti.
* Perdarahan ( > 10 % EBV ).
* Trauma karena pembedahan –ringan sampai besar
(3-10ml/kg/jam).
* Continuing/ongoing loss
– Pipa lambung,drainase luka,
- Drainase rongga tubuh.

4 ml/kg/jam – 10 kg bb pertama.
+ 2 ml/kg/jam – 10 kg berikutnya.
+ 1 ml/kg/jam – untuk berat badan diatas 20 kg.
Contoh:
Bayi 8 kg. – kebutuhan cairan rumatan = 8 x 4 = 32 ml/jam.
Bayi 12 kg. – kebutuhannya = 10 x 4 = 40 ml/jam
2 x 2 = 4 ml/jam
44 ml/jam
Bayi 25 kg. – berapa kebutuhan cairan rumatan ?


Natrium - 2 – 4 mEq/kg/hari.
Kalium - 1 – 3 mEq/kg/hari.
Chlorida - 2 – 3 mEq/kg/hari.
Calcium - 40 – 80 mEq/kg/hari.
Phosphor - 20 – 45 mEq/kg/hari.
Magnesium - 6 – 10 mEq/kg/hari.

Cadangan glikogen sedikit.
* kebutuhan kalori 30 – 100 kcal/kg/hari.
Jadwal puasa.
* 10 – 20 g/kg/hari.
* mulai dengan glukosa 5% -- 20%disesuaikan
dengan jam pembedahan.
Infus mengandung glukosa
ASUS
Highlight
ASUS
Highlight

Poikilotermis.
* luas permukaan tubuh > dewasa.
* lemak subkutan minimal.
* kehilangan panas
- Radiasi
- Konveksi
- Evaporasi,
-Konduksi.


Non-shivering thermogenesis.(sebagai kompensasi produksi panas bila suhu turun).Kompensasinya dengan oksidasi “brown fat” – konsumsi O2 >
- asam lemak bebas> - asidosis metabolik
Suhu sekitar netral.
* selimut,topi,matras hangat.
* cairan infus hangat.
* suhu kamar bedah.
ASUS
Highlight
ASUS
Highlight


Psikotrauma - gangguan perilaku.
Usia 2 – 5 tahun psikis labil.
Nyeri fisik :
* jarum suntik.
* luka pasca bedah.
* penggantian bebat
Rasa tidak nyaman :
* pusing , mual , muntah.
* infus , kateter , drain, pemasangan nasogastric tube, ventilasi mekanik.
Stress emosional :
* pisah dari orangtua.
* bau2an , suara2 di RS/kamar bedah.
* penglihatan yang mengganggu


PERSIAPAN PRA-ANESTESI.
PELAKSANAAN ANESTESI.
PERAWATAN PASCA-ANESTESI.

ANAMNESA/HETEROANAMNESA.
PEMERIKSAAN FISIK & LABORATORIK.
* masalah anestesi.
* masalah pembedahan.
* masalah penyakit utama/penyerta.
TINDAKAN2 PENCEGAHAN PENYULIT.
TEHNIK & OBAT ANESTESI.

A. PERSIAPAN PASIEN
1. ANAMNESA / Kunjungan pra-anestesia
2. PEMERIKSAAN FISIK
3. PEMERIKSAAN PENUNJANG
B. PERSIAPAN ALAT DAN OBAT

Riwayat kesehatan ibu selama hamil, adanya pemakaian obat-obatan ataupun alkohol, merokok, diabetes dan infeksi virus
Pemeriksaan kehamilan sebelum melahirkan : usg
Umur kehamilan saat melahirkan bayi, nilai APGAR bayi
Adanya infeksi saluran nafas atas saat ini, trakeobronkitis, asma, riwayat snooring, episode sianosis
Posisi bayi/anak saat tidur ( terlentang, miring lateral, telungkup)

Riwayat perawatan di rumah sakit sebelumnya
Kelainan kongenital, kelainan metabolisme
ataupun adanya suatu sindroma
Riwayat perkembangan dan pertumbuhan pasien
Adanya retardasi mental
Riwayat operasi dan anestesi sebelumnya
Riwayat alergi
Kecenderungan perdarahan bila terjadi luka
Riwayat penggunaan obat-obatan saat ini

Status fisik secara umum, meliputi kesadaran, tingkat aktivitas pasien, interaksi sosial, warna kulit, tonus otot, kelainan kongenital yang ada, ukuran dan lingkar kepala
Vital sign, tinggi dan berat badan, status nutrisi, status hidrasi
Kondisi gigi, kelainan craniofacial, ataupun adanya tonsil yang besar yang dapat menyulitkan penguasaan jalan nafas
Tanda infeksi saluran nafas atas atau asma. Sekresi di jalan nafas
Pemeriksaan bunyi jantung ( adanya murmur)
Kemungkinan lokasi untuk pemasangan akses intravena
PEMERIKSAAN FISIK


DL rutin tidak perlu dilakukan pada anak yg sehat dengan operasi minor
Hb ≥ 10 g% Pemeriksaan penunjang sesuai indikasi : ◦ Faal hemostasis susp. Gangguan pembekuan darah dan
operasi dgn perdarahan banyak ◦ Urinalisis jarang diperlukan ◦ Fungsi ginjal : BUN & SC ◦ Fungsi liver Pada pasien yang diketahui adanya risiko kelainan hati Menjalani prosedur yang akan mengganggu fungsi hati
◦ Ro thorax ◦ EKG ◦ Serum elektrolit, albumin ◦ Gula darah
ASUS
Highlight

USIA LAMA PUASA (JAM)
MAKANAN PADAT MAKANAN CAIR
< 6 BULAN 4 2-3
6-36 BULAN 6 2-3
> 36 BULAN 8 2-3
Asi dapat diberikan s/d 4 jam preoperative
ASUS
Highlight
ASUS
Cross-Out
ASUS
Underline

ALAT :
1. Masker + jackson reese
2. Oropharyngeal tube
3. Endotracheal tube
4. Laryngoscope + blade
5. Plester fiksasi
6. LMA
7. Bantal intubasi + bantal donat
8. Mesin anestesi + sumber oksigen
9. Suction catheter
10. EKG electrode +
monitor
11. Stetoskop prekordial
12. Saturasi O2
13. Tampon + Mcgill
14. Nasogastric tube
15. Salep mata + plester
16. Temperatur
17. Matras penghangat
18. Penghangat infus

Obstruksi jalan nafas & expansi paru <. * bantal punggung.
* dead space mekanik <. * sistim anestesi inhalasi – ringan,tanpa katup.
Kardiovaskuler & hemodinamika. * siap Sulfas Atropin.
* pediatric infus set + burette.
* observasi perdarahan teliti.
* pembedahan pagi.
Pencegahan hipo/hipertermi. Pencegahan trauma psikis. * pendekatan psikologis.
* pendekatan farmakologis.

Pembedahan jalan nafas & posisi telungkup.
* intubasi trachea.
Perdarahan.
* siap darah.
* infus lancar.
* perkiraan perdarahan cermat – kassa ditimbang.
Pembedahan darurat.
* rehidrasi/transfusi.
* terapi oksigen.
* pengosongan lambung.

PREMEDIKASI.
INDUKSI.
RUMATAN ANESTESI.

SEDASI
ANALGESIA
PENGERING JALAN NAFAS
VAGOLITIK
ANTIEMETIK
AMNESIA

SEDATIVA/AMNESIK.
* Benzodiazepines – diazepam , midazolam.
* Antiemetika – dehydrobenzperidol (DHBP).
* Antihistamin – promethazine (Phenergan).
ANALGETIKA.
* Narkotik – morphine , pethidine,fentanyl
VAGOLITIK/PENGERING.
* Sulfas atropine.
* Scopolamine.
ASUS
Highlight
ASUS
Highlight
ASUS
Highlight
ASUS
Underline
ASUS
Underline
ASUS
Underline
ASUS
Underline
ASUS
Underline

Pasien relatif kooperatif :
Diazepam oral 0.2-0.3 mg/kgbb
Ketamin oral 4-6 mg/kgbb
Fentanyl “lolypop” 5-15 μg’kgbb pasien dgn nyeri (trauma) atau prosedur operasi kelainan jantung
Pasien tidak koopertif :
Midazolam im 0.1-0.15 mg/kgbb
Ketamin im dosis rendah 2-3 mg/kgbb
Premed antikolinergik im tidak dianjurkan iv saat induksi
Bila resiko refluks astroesofageal : metokloperamide 0.1 mg/kg + simetidin 7.5 mg/kg atau ranitidin 2 mg/kgbb iv)
Obat-obat preoperative lain tetap diminum : obat asma, epilepsi, hipertensi, dll
ASUS
Highlight
ASUS
Highlight
ASUS
Highlight

< 1 TAHUN.
* inhalasi overface.
*parenteral.
> 1 TAHUN.
* inhalasi overface + orangtua
* parenteral – intramuskuler , intravena.
* perrectal.

Induksi inhalasi : halotan, sevoflurane Yang lain tidak bisa karena berbau,
menimbulkan batuk, menahan napas dan laringospasme (desflurane atau isofurane)
Induksi intravena : ketamin, penthotal, propofol
Induksi intramuskular : pasien yang sangat tidak kooperatif dan mengamuk / gelisah ketamin
Induksi perrektal : ketamine, pentotal, midazolam
ASUS
Highlight
ASUS
Highlight
ASUS
Highlight
ASUS
Highlight

PER-INHALASI.
* ether.
* halothane. + O2
* enflurane.
* isoflurane.
PAR-ENTERAL.
* ketamine yang mengakibatkan dissociative
anesthesia.

Ringan sesuai dengan resistensi pernafasan – / < Dead space mekanik minimal. Contoh : * Schimmelbusch mask. * Jackson Rees
apparatus. * Ayre’s T-piece. * Pediatric Circle System. Perlengkapan lain. * laryngoskop. * jalan nafas orofaring. * penghisap. * pipa endotrakheal. * obat2 darurat.

1. MONITORING DURANTE OP
a. Airway tetap bebas ( ETT terfiksasi dengan baik)
b. RR, amplitudo, suara nafas, saturasi O2, ETCO2
c. Perfusi, Nadi, tekanan darah, EKG, stetoskop prekordial
d. Produksi urine 0,5 cc/kg/jam dan keseimbangan cairan
e. NGT
f. Suhu (axilla , rectal , oesophagus).
g. Gula darah
hipoglikemia diterapi dengan 1-3 ml/kg glucose 20% i.v dalam 5 menit
ASUS
Highlight
ASUS
Highlight

RR HR TD
sistolik
TD
diastolik
Neonatus 40 140 65 40
12 bln 30 120 95 65
3 th 25 100 100 70
12 th 20 80 110 60

Bradikardia :
◦ Bila karena hipoksia diterapi dengan cara ventilasi & oksigenasi adekuat akan mengembalikan denyut jantung
◦ Bila karena Reflek vagal : contoh pada operasi mata, usus diterapi dengan cara meminta operator berhenti sementara dan pemberian Sulfas Atropin 0,5 mg (2 ampul) secara intravena
◦ Bila karena peningkatan Tekanan Intra Kranial maka dilakukan hiperventilasi, diuretik, operator diminta untuk berhenti sementara
ASUS
Highlight
ASUS
Highlight
ASUS
Highlight

Endotracheal Tube terlepas, kinking maka dilakukan fiksasi yang baik ,dan pemasangan tampon
Perdarahan
Dehidrasi harus dilakukan reasses dehidrasi yang baik dan rehidrasi sehingga harus diperhatikan cairan maintenance + evaporasi
Nyeri diberikananalgetika
Bila Hipotermi maka pasien dihangatkan dengan bantal penghangat, penghangat infus
Bila Hipertermi maka dilakukan kompres dingin, buka pembungkus extremitas, suhu ruangan didinginkan




• REGIONAL
• KOMBINASI REGIONAL dan GENERAL

RA only :
Reduces the risk of post operative apnoea in pre mature children.
Over night monitoring must be there
In older age group RA can not be done alone.

Safe, reliable technique in infants at risk of apnoea, bradycardia and desaturation after GA
Good alternative for day care surgeries
Minimal risk of postoperative respiratory depression
Limited stress response to surgery
Cost effective
Keuntungan Regional anestesi:

KOMBINASI RA + GA :
Usually RA for anaesthesia and also for post operative pain relief
Single caudal
Continuous epidural / caudal
Peripheral nerve blocks
Field blocks
Local infiltration.

Contra-indications:
Parent refusal
Sensory nervous system diseases
Serious sepsis
Bleeding disorders
Vertebral malformations
Previous surgery on spines
Allergy

Acceptable environment for performing regional blocks:
Minimal mandatory monitoring
Anaesthetic and emergency drugs
Resuscitation equipments
Trained anaesthesiologist
Trained staff
iv line in situ

Most common regional block in children
Simple to perform
Easily adaptable to ambulatory anesthesia practice
Greatly decreases risk of reflex laryngospasm

Sacral hiatus easy to identify Palpable large bony processes on each side of
hiatus called cornua Hiatus covered by sacrococcygeal membrane Dural sac may extend to S3 or S4 in infants
(short distance between hiatus and dural sac)


Lateral decubitus position
Palpate coccyx
Move finger gently from side to side and proceed in cephalad direction
First double bony protuberance encountered are sacral cornua which define the sacral hiatus


Major complications rare ◦ Intravascular injection with systemic toxicity
◦ Dural puncture causing high spinal blockade
◦ Infection (especially after interosseous puncture/penetration)

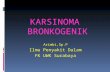
CAUDAL ANESTESI

Caudal block procedure. A, Insertion of the needle at right angles to the skin in relation to the coccyx (1) and the sacrococcygeal membrane (2). B, Cephalad redirection of the needle after piercing the sacrococcygeal membrane.

Anatomy and physiology: The spinal cord and dural sac of infants younger
than 1 year of age end at a lower level Volume of CSF a. 10 mL/kg in neonates b. 4 mL/kg in infants weighing less than 15 kg c. 3 mL/kg in children d. 1.5 to 2.0 mL/kg in adolescents and adults
50% CSF volume is located within the spinal subarachnoid space versus 25% in adults
Lower CSF hydrostatic pressure Children older than 5yr behave like adults after
spinal anaesthesia, whereas younger patients remain hemodynamically stable, without significant hypotension or bradycardia

Indications: Inguinal hernia repair in former preterm infants
<60 weeks of postconceptual age
Elective lower abdominal or lower extremity surgery
Cardiac surgery or cardiac catheterization (controversial)

Spinal anaesthesia: Technically similar to adults. Not very commonly done procedure, must have IV access, 1.5 inch 25 G beveled needle.
Dose: 0.3-0.6 mg/kg of 0.5 % Bupivacaine heavy. Higher the age, lower the dose and vice versa

Improved surgical outcomes: ◦ Decreased stress response ◦ Fewer episodes of hypoxia ◦ Decreased cardiac morbidity ◦ Decreased pulmonary infections ◦ Decreased thromboembolic events ◦ Decreased blood loss ◦ Faster return of GI function

Drugs Used: ◦ Ropivacaine/Bupivacaine
◦ 2 - Chloroprocaine
◦ Morphine
◦ Clonidine

Complications: ◦ Intrathecal injection High block
Postdural puncture headache
◦ Intravascular injection/Local anesthetic toxicity ◦ Sympathectomy Hypotension
Bradycardia

Complications: ◦ Opioid –induced respiratory depression
◦ Damage to neural structures
◦ Infection
◦ Epidural Hematoma paraplegia
< 1 in 150,000
Usually associated with anticoagulation

Epidural block procedures: sacral intervertebral approach (1), lumbar approach (i.e., midline route) (2), and thoracic approach (i.e., midline route) (3).

PERIPHERAL BLOCKS

Penile block (Dalen’s sub pubic block):

Provides analgesia after superficial surgery of penis ◦ Circumcision
◦ Meatotomy
Blocks both dorsal nerves at base of penis ◦ Anesthesia to distal two-thirds of penis

Usually performed by surgeon
Avoid epinephrine ◦ May lead to ischemia of tissue
Complications: ◦ Intravascular injection
◦ Hematoma formation

Simple subcutaneous ring block at the root of the penis is sufficient but duration is only for 2-4 hrs.

UPPER LIMB BLOCKS

Brachial plexus block:
It can be sole anaesthetic or as an adjuvant to GA or for post OP analgesia or for sympathetic blocks. It should not be used for trivial reasons. Age is not a contra-indication for this block. Must be associated with GA. PNS or USG can be used to locate the nerves.

Inter scalene block:

Supra clavicular block:

Axillary block:

Axillary approaches to the brachial plexus: classic approach (A) and transcoracobrachialis approach (B), indicating the pectoralis major muscle (1), axillary artery (2), and coracobrachialis muscle (3).

LOWER LIMB BLOCKS

Femoral nerve block:

LATERAL CUTANEOUS NERVE OF THIGH (LCNT) BLOCK:


Simple Block
Good pain relief for hernia repair, hydrocelectomy and orchiopexy
Can be done at beginning of case for both intraop and postop analgesia
May be done intraop under direct visualization


Pemantauan sistim pernafasan & kardiovaskuler. Temperatur – > 35 derajat Celsius. Posisi miring/semiprone. Nyeri pasca-bedah. Bisa memakai fentanyl, ketorolak, acetaminopen
rektal, pethidin Antisipasi penyulit pasca-bedah. * edema larynx. * laringspasme * aspirasi. * perdarahan. Kebutuhan cairan , elektrolit , kalori.


Related Documents